













Children Don’t Need COVID Vaccines
I may be just a mom to most people, but I’m not alone in thinking children don’t need COVID vaccines.
Marty Makary, MD, MPH and a professor at Johns Hopkins School of Medicine weighed some of the pros and cons, and found there is no benefit for young, healthy children:
“I would not recommend a two-dose vaccine regimen for a healthy child ages 0 to 12 years until we have more data. Each parent will have to assess their own child’s individual risk, but in my opinion, the case to vaccinate young healthy kids is not compelling right now.”
Pediatricians like Richard Malley, MD, of Harvard, and Adam Finn, MD, PhD, of the University of Bristol, have passionately written to not “use precious coronavirus vaccines on healthy children.”
Physician epidemiologist and associate professor Johns Hopkins School of Public Health, Stefan Baral and two colleagues wrote a BMJ Opinion “Covid vaccines for children should not get emergency use authorization,” which correctly points out:
“An emergency use authorization (EUA) in the US requires that an intervention address a serious or life threatening condition, and for known and potential benefits of the intervention to be balanced against the known and potential harms.”
Listen to your intuition
Throughout all of this, my biggest concern has always been that the vaccine itself may be more dangerous to children, than the actual virus.
Given that every medical treatment or procedure has inherent risks, both short term and long term that may not be detected for weeks or months, it doesn’t make sense to inject our children with something much, much more harmful to them.
What we know right now about the COVID vaccines:
- No long-term safety or efficacy data (Might be ok for an 80 year old, but NOT OK for a child)
- Not FDA approved
- Sample sizes too small to detect serious rare adverse events (clinical trial only studied 1,131 adolescents ages 12-15, and only followed up with 660 teens for 2 months before giving to millions??)
- Clinical trials won’t technically end until at least 2023
- Individual risk outweighs individual benefit for the vast majority of children
- Risk of Anaphylaxis (2.47 per 10,000 vaccinations)
- Increases risk for heart inflammation (myocarditis / pericarditis)
- Increases risk for blood clots and thrombotic events, including stroke
Under an Emergency Use Authorization, the FDA may allow the use of unapproved medical products:
“To diagnose, treat, or prevent serious or life-threatening diseases or conditions when certain statutory criteria have been met, including that there are no adequate, approved, and available alternatives.”
Except COVID-19 is not “a life-threatening disease or condition” in children at all. This political misuse of the authorization is a detriment to our children.
This isn’t public health at all, this is literally putting the public at risk.
Historically, FDA approval is not something we can hang our hat on, either. This study found that after approval, 1 in 3 drugs are associated with post-market safety events, including withdrawal, boxed warnings, and safety communications.
These are CHILDREN.
This is why we should exercise extreme caution when it comes to young, healthy children whose lives are not in danger, who have a long life ahead of them (and therefore are risking more when it comes to negative, long-term health effects). Remember thalidomide?
Our government agencies don’t replace or upend our own responsibility to properly care for, and defend our children’s health. It’s up to us to make sense of this highly political move to vaccinate kids–because it’s not scientifically or ethically-based.
These are my ten reasons children don’t need COVID vaccines:
1. Children Are Not At Risk For Severe COVID Disease
Children are not where this pandemic is at. I think most people realize that, but just in case, here are all the stats:
As of June 9, there have been 33.4 million SARS-Cov-2 infections reported in the United States since early 2020, and of those infections, there have been 586,659 deaths from, or just with, the SARS-CoV-2 virus.
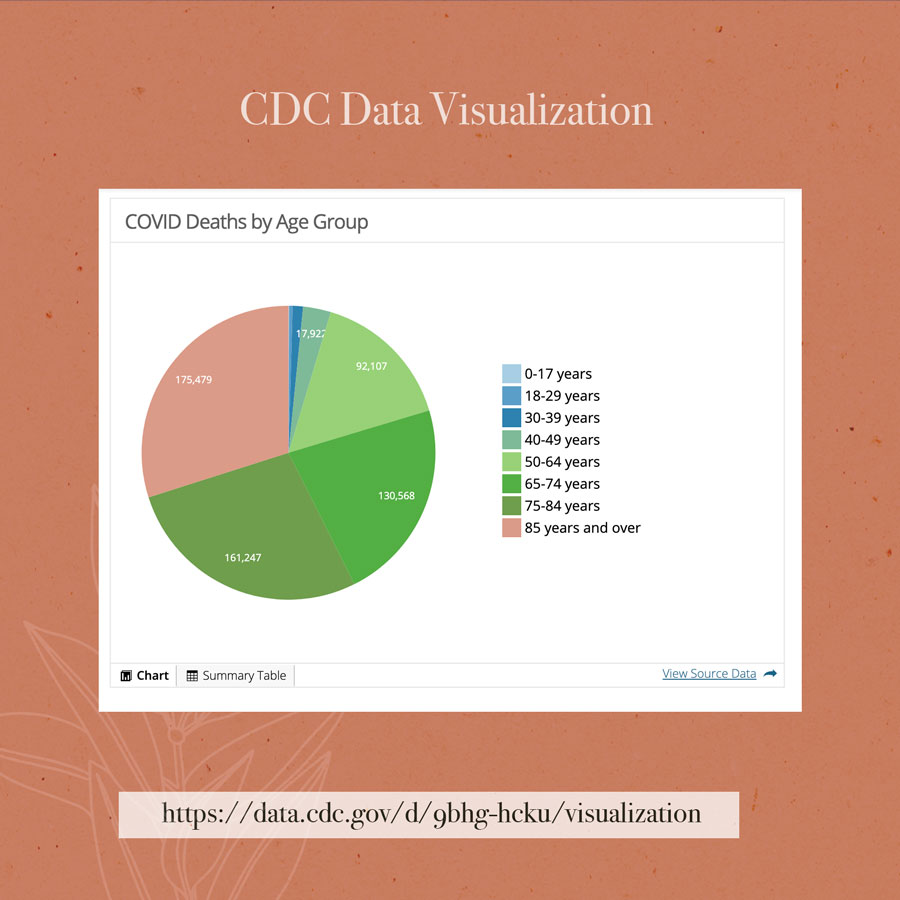
Eighty percent of the COVID deaths were in people over the age of 65, and 95% of deaths had on average 4.0 additional conditions of causes per death, including pre-existing comorbidities such as:
- hypertensive diseases (115,094)
- diabetes (93,474)
- ischemic heart disease (64,978)
- chronic lower respiratory disease (51,906)
- malignant neoplasms (28,121)
- obesity (23,658)
- Alzheimer’s Disease (20,977)
- intentional and unintentional injury, poisoning, and other adverse events (11,858)
Only 5% of all COVID-19 deaths was COVID-19 listed as the only cause on the death certificate.
It is estimated approximately 30% of coronavirus infections are completely asymptomatic (and therefore not reported).
The median infection fatality rate (based on 51 locations) is estimated to be 0.27% (corrected 0.23% for seroprevalence.)
For people younger than 70 years old, the infection fatality rate of COVID-19 across 40 locations with available data ranged from 0.00% to 0.31% (median 0.05%).
Read that again.

Not to negate the sadness and seriousness of elderly deaths, it seems like people have an unreasonable assumption that COVID-19 must be dangerous in children or young adults, because it’s dangerous in elderly adults, and that’s just not the case.
Or that it’s children’s job to protect adults, which again, it’s not.
Out of the 586,659 COVID-19 deaths, only 314 deaths were recorded in 0-17 year olds, which is 0.05% of all COVID deaths.
If you go by the CDC’s pandemic planning scenarios which are estimates, the infection fatality rate for people under the age of 20 years old is: 0.002%.
This is an extremely low mortality rate for any infection, and that’s a good thing. For example, in the same time period, the same age group experienced:
- 765 non-covid pneumonia deaths
- 183 influenza deaths
From 2019 mortality statistics, children 14 and under died from:
- 401 other and unspecified infectious and parasitic diseases and their sequelae
- 401 influenza and pneumonia
- 366 other diseases of the respiratory system
- 249 septicemia
- 219 intestinal infections
This is with a vaccination program for both pneumonia and influenza in place, which have been steadily increasing flu mortality rates in children for years.
Keep information in perspective:

If you are afraid of your child contracting SARS-CoV-2 and dying or being severely injured, then you should be more concerned of the leading causes of death in children, which are statistically more likely to occur. Odds are odds. It doesn’t matter if something is contagious or not, your odds of dying don’t know the difference.
According to the CDC, in 2019 the leading causes of deaths in ages 0-14 were:
- 10,381 died from certain conditions originating in the perinatal period
- 5,098 died of congenital anomalies
- 3,907 died of accidents / unintentional injury
- 2,785 died of symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (R00-R99) (SIDS would go here)
- 1,115 died of malignant neoplasms
- 893 children died of homicide
- 645 children died from accidental submersion and drowning
- 93 children died from complications of medical and surgical care
I, like you, do everything I can to keep my children alive AND healthy. But I won’t keep them from living life to their fullest potential. That’s exactly why I promote informed consent, and encourage vaccine safety surveillance.
Vaccines are not tested for mutagenicity or carcinogenic potential (section 13.1 on every vaccine insert), are not monitored for long-term health effects. There is limited data as to their overall safety.
Bottom Line: Because children are clearly not at risk for severe disease, it makes no sense to subject them to a medical procedure that may have long term health implications for them, that isn’t FDA approved, whose actual safety profile is unknown, and which isn’t designed to benefit them at all.
Conversely, the long lasting immunity from a SARS-CoV-2 infection (this study showed 10 months of protection, and counting) will protect them from variants, may even be lifelong (because antibodies aren’t all there is) to protect them precisely when they’re elderly and vulnerable, and will protect others, too.
Herd immunity is much more stable and long lasting with natural infection, compared to vaccine-induced immunity, which wanes, can cause a linked epitope suppression, and leads to a higher susceptibility to all infections.

2. COVID Vaccines Don’t Exactly Stop Transmission, Either
While mainstream news is probably running around saying “yes they do!” We of course know the vaccines don’t prevent infection in every case.
We have ‘breakthrough cases’, we even have fully vaccinated people dying of COVID-19, the very disease the vaccine is supposed to prevent. Plus, don’t forget all vaccines wane over time. So not only does it fail at preventing transmission, the vaccine also fails at preventing COVID-19. No matter how it’s spun, this is evidence of vaccine failure.
The CDC has stopped tracking breakthrough cases, and so are some States now, like California. Reporting on ‘Breakthrough’ cases may undermine confidence in the vaccine program, but it’s not science based if extremely pertinent data such as this is no longer collected.
Here are just a few of the recent headlines:
Maine says 8 vaccinated residents died ‘with COVID-19’
‘Breakthrough’ COVID death: Fully-vaccinated California woman dies from virus
After Fully-Vaccinated Father Dies of COVID-19, Family Hopes Story Raises Awareness
County Confirms 1st Death of Fully Vaccinated San Diegan in So-Called Breakthrough Case
A fully vaccinated cruise set sail in the Caribbean. Two passengers just tested positive for covid.
Vaccinated Los Angeles doctor diagnosed with COVID-19, warns about breakthrough cases: report
More Than 500 Breakthrough Infections Reported in Mass. in Under 3 Weeks
Vaccines also don’t affect case fatality rates. According to the CDC, they tracked 10,262 SARS-CoV-2 vaccine breakthough infections (before deciding they would stop tracking them) and among those cases:
“Based on preliminary data, 2,725 (27%) vaccine breakthrough infections were asymptomatic, 995 (10%) patients were known to be hospitalized, and 160 (2%) patients died.”
So, despite vaccination, 2% of the breakthrough cases died of COVID-19. We also don’t know how many COVID-vaccinated people have died of other causes, and whether their overall mortality has been higher so far in 2021, but I’m guessing so since our overall mortality was very high in January, after a vast majority of the elderly got their first doses, and some got their second doses.

All vaccines wane over time, and the COVID vaccines will as well. Are you going to get annual boosters? Are you going to require your children to get annual boosters? With something that may cause anaphylaxis or heart failure?
Studies have shown that getting annual flu vaccinations actually increase your risk of getting influenza.
Pertussis vaccination is associated with a phenomena called linked epitope suppression, which causes children who have been vaccinated against pertussis to have a higher lifetime susceptibility to the infection. This is why as much as 90% of annual pertussis cases are in children who have been vaccinated against pertussis.
Bottom line: Vaccines won’t guarantee zero transmission in an open-ended duration of time–and then what? You’re going to vaccinate every year?? No, way. You are compounding your risks, again with no benefit for your child.
Vaccination may actually increase your child’s lifetime susceptibility to coronavirus infections. We won’t know until the trials end, and everyone reports their breakthrough infections / hospitalizations / deaths to VAERS, and cross our fingers the CDC reports things transparently.
3. Majority of Cases are Asymptomatic or Mild
In total, around 80% of confirmed coronavirus infections are clinically mild. The CDC estimates that 30% of cases are completely asymptomatic, and therefore not even detected. This is irrespective of age.
Reserve vaccination for a microbe that is really deadly and scary, an ‘imminent danger’: but this just ain’t that--not for everyone.
Nor should we pretend it is scary for everyone.
There are several biological reasons why children typically have more mild infections, compared to adults, and one may be because of an enzyme called ACE2. Angiotensin-converting enzyme 2 (or ACE2 for short) is the receptor that the SARS coronavirus binds to in order to infect its host. The spike protein competes with the enzyme for binding.
Children have the least number of ACE2 receptors compared to all other age groups. According to this study:
“Among a cohort of 305 patients aged 4 to 60 years, older children (10-17 years old; n = 185), young adults (18-24 years old; n = 46), and adults (≥25 years old; n = 29) all had higher expression of ACE2 in the nasal epithelium compared with younger children (4-9 years old; n = 45), and ACE2 expression was higher with each subsequent age group after adjusting for sex and asthma.”
This may be why less than 10% of total infections have occurred in children ages 5-17 years of age. Among the first 149,082 US cases, around 1.7% of the cases were in children under 18 years.
A targeted screening approach in Iceland found SARS-CoV-2 in 6.7% of children younger than 10 years old (n = 564) compared with in 13.7% of people aged 10 years or older (n = 8635).
The ratio of cases in children may be slightly higher now (around 14%), but mainly because the CDC is not keeping track of ‘breakthrough cases’, and they are recommending that COVID-vaccinated people can skip routine testing altogether. Fewer testing = fewer cases.
But even so, throughout this pandemic, a large proportion of cases have been asymptomatic, and remained asymptomatic.
A systematic review found that:
Among the 43 studies using PCR testing, the proportion of persons who tested positive but had no symptoms at the time of testing ranged from 6.3% to 100%, with a median of 65.9% (IQR, 42.8% to 87.0%).
The proportion of persons who tested positive and remained asymptomatic ranged from 6.3% to 91.7%, with a median of 42.5% (IQR, 29.6% to 77.8%)
Of the 19 longitudinal studies, 14 provided information on the evolution of symptomatic status:
“Among persons who tested positive but had no symptoms at the time of testing, the proportion who remained asymptomatic during a follow-up period ranged from 11.1% to 100%, with a median of 72.3% (IQR, 56.7% to 89.7%).”

And according to a mass screening program performed in Wuhan, China on 10 million people between the ages of 10 and 89, the researchers found only 300 asymptomatic cases and none of them were infectious:
“No “viable virus” in cultures from asymptomatic samples.”
“The asymptomatic positive rate was lowest in participants aged under 17 and highest in those over 60. Further swab testing of 1174 close contacts of the 300 asymptomatic positive cases were all negative.”
The 300 asymptomatic cases discovered in the screening program did not pass the virus on to any close contacts.
Bottom Line: We should feel pretty darn good that most infections are mild or asymptomatic, and that one bout of illness yields long-term immunity. Getting a vaccine now, just postpones the inevitable.

4. Kids Don’t Spread the Virus As Much as Adults
So far every epidemiological study has found that kids are the opposite of super-spreaders. The younger age groups spread the least virus, study after study shows.
It is well known that the majority of transmission occurs in homes (including nursing homes)–not outside, not at parks, not at schools, not at restaurants or shopping centers, not walking down the street, not riding a bike–but even so, you still only have about a 10% chance of getting the virus from a person you live with. There is an even lower chance of getting SARS-CoV-2 from a child inside a home.
A meta-analysis of household transmission clusters found:
“Only 8 (3.8%) transmission clusters were identified as having a pediatric index case.”
And…
“The secondary attack rate in pediatric household contacts was lower than in adult household contacts (RR, 0.62; 95% CI, 0.42-0.91).”
A study of a half a million people in India found that a very small minority of people are responsible for spreading the virus:
“The researchers found that 71% of infected individuals did not infect any of their contacts, while a mere 8% of infected individuals accounted for 60% of new infections.”
“The researchers found that the chances of a person with coronavirus, regardless of their age, passing it on to a close contact ranged from 2.6% in the community to 9% in the household.”
A study in Israel followed hundreds of thousands of youths ages 0-19 years and found that the age group 0-9 years had the lowest rates of infection and the lowest spread compared to all other groups studied:
Our study’s findings suggest that children aged 0 to 9 years did not have substantial rates of SARS-CoV-2 infection during school attendance periods, and it may be assumed that they did not have a substantial role in COVID-19 spread either during this period.
A 40,000-person study in Iceland found that children under 15 were about half as likely as adults to be infected, and only half as likely as adults to transmit the virus to others.
A study performed in Italy looked at whether schools contributed to a “second wave” of cases by analyzing 21 Italian regions. The results were that:
“From September 12 to November 7 2020, SARS-CoV-2 incidence among students was lower than that in the general population of all but two Italian regions. From August 28 to October 25 in Veneto where school reopened on September 14, the growth of SARS-CoV-2 incidence measured across all age groups was lower in school age individuals, maximal in 20-29 and 45-49 years old individuals.”
Same thing was observed in Ireland:
The results moreover echo the experience of other countries, where children are not emerging as considerable drivers of transmission of COVID-19.
Not everyone will transmit virus to another person. A CDC study did contact tracing on two hairdressers: while the stylists were masked at their salon, they didn’t pass their SARS-CoV-2 infection to any of their 139 clients. At home, stylist A did pass infection to her 4 close contacts at home, while stylist B did not pass infection to her 2 close contacts at home.
Caution: Be wary of non-epidemiological studies like this, which used PCR to detect viral nucleic acid (not infectious virus) in the nasopharynx in various age groups to then conclude that ‘children should be immunized.’ There is no way to know if the viral fragments mean anything because they couldn’t prove infectiousness, or epidemiological spread from these children.
Oh and the “conflicts of interest” section is a doozy: It’s funded by NIAID (Fauci) and the authors are all heavily funded by Big Pharma. Always read the fine print:

Bottom Line: There is no evidence that kids are super-spreaders and in fact, all available evidence shows the complete opposite picture. Trust the science, aye? And don’t fall for the Big Pharma word snot pretending to be science. Always read the “conflicts of interest” section of every study to determine how legitimate and objective the study may or may not be.
Tip: Don’t ask a barber if you need a hair cut.

5. We Aren’t Supposed To Vaccinate Someone Who May Have Had COVID
To this day, the official stance of the CDC is “everyone must get vaccinated,” irrespective of whether they had a prior infection. And this is a dangerous precedent. Not only have we never done this, but vaccinating people who have recovered from the illness in question, or vaccinating potentially asymptomatic individuals, increases a person’s risk for severe adverse reactions.
There is a strong possibility that many, many children had an asymptomatic coronavirus infection that was never detected, and going onto vaccinate them indiscriminately may increase their risk of harm.
This observational study in the United Kingdom of health care workers found that:
“Prior COVID-19 infection but not ongoing Long-COVID symptoms were associated with an increase in the risk of self-reported adverse events following BNT162b2/Pfizer vaccination.”
Another observational study from the UK found that:
“Systemic side-effects were more common (1·6 times after the first dose of ChAdOx1 nCoV-19 and 2·9 times after the first dose of BNT162b2) among individuals with previous SARS-CoV-2 infection than among those without known past infection.”
A survey conducted through Poland’s National Vaccination Program found that younger age groups (19-30 y vs. all higher age groups) and people who had a previous coronavirus infection were more likely to experience more severe side effects after the first dose of the COVID-19 vaccine.
A self-reported vaccine recipient survey found that:
A prior COVID-19 infection was associated with an increased risk of any side effect (risk ratio 1.08, 95% confidence intervals (1.05-1.11)), fever (2.24 (1.86-2.70)), breathlessness (2.05 (1.28-3.29)), flu-like illness (1.78 (1.51-2.10)), fatigue (1.34 (1.20-1.49)) and local reactions (1.10 (1.06-1.15)). It was also associated with an increased risk of severe side effects leading to hospital care (1.56 (1.14-2.12))
Not only are there associated risks with vaccinating people who have recovered from prior infection, there is also data to support that people who had natural infection get reinfected at the same rate as those who had natural infection and are vaccinated (so no benefit), while the cumulative incidence is slightly higher in previously uninfected, vaccinated subjects (See figure 3).
Bottom Line: Science has really gone out the window with indiscriminate vaccination of an entire population during a pandemic.
It’s unprecedented, it’s risky, and it’s not to be confused with science or common sense. Remember that time you got chicken pox and then you got a chicken pox vaccine? Me neither.
The fact that so many children may have had subclinical or completely asymptomatic infections, and that evidence is pointing to prior infection increases risk for adverse reactions, should compel every parent to at least get that antibody test before considering a COVID vaccine for their child.

6. Actual Data On COVID Infections in Children Don’t Support Routine Vaccination
Looking at the available information on children and SARS-Cov-2 infections from 2020, of 1.2 million laboratory confirmed infections in 0-17 year olds, 2.3% resulted in hospitalization, 0.8% of admissions into an ICU.
Fewer than 0.1% of laboratory confirmed infections resulted in death.
If you go by the CDC’s pandemic planning scenarios which are estimates and figure in the unidentified asymptomatic infections, the infection fatality rate for people under the age of 20 years old is 0.002%.
A meta-analysis looked at pediatric mortality from COVID-19, and found that of 274,647 pediatric infection without comorbidities, only 77 (0.03%) died, compared to 134 (1.5%) of the 8,960 children with pre-existing conditions died during the course of their SARS-CoV-2 infection.
Of the children who developed severe illness from COVID-19, most have had underlying medical conditions.
These are not apples to apples. A child with no comorbidities, or pre-existing conditions is at the lowest of the lowest risk of all groups, and should not be put at unnecessary risk with zero benefit.
The recent CDC MMRW report on hospitalizations of adolescents aged 12-17 with confirmed COVID-19 from March 1 to April 24 documented:
- 204 adolescents “likely” to be hospitalized for COVID-19 (their language, not mine)
- 70% of the adolescents had ≥1 underlying medical condition
- Less than 5 percent required mechanical ventilation
- Zero deaths
Bottom Line: Children make up the tiniest fraction of hospitalizations and deaths, so small that if it was any other year we would never consider vaccinating them.
Conversely, vaccinating millions and millions of children will produce exponentially more severe reactions and deaths than the virus ever would.
Just because there are talking heads that encourage or coerce you to vaccinate your child, does not mean they are in imminent danger, does not mean they are at risk, does not mean they will play a meaningful role in the spread of coronavirus at all–because all available evidence shows otherwise.
7. MIS-C In Children Doesn’t Warrant Mass Vaccination
Maybe you have heard about MIS-C, or multisystem inflammatory syndrome. It’s an extremely rare but serious complication of a SARS-CoV-2 infection (or vaccination) in children as well as adults.
MIS-C is a condition where different body parts can become inflamed, including the heart, lungs, kidneys, brain, skin, eyes, or gastrointestinal organs. Symptoms may include fever and various symptoms, including abdominal (gut) pain, vomiting, diarrhea, neck pain, rash, bloodshot eyes, or feeling extra tired.
From May 2020 to June 2021, there have been 4018 cases of MIS-C, of which 36 children have died.
The CDC writes:
“We do not yet know what causes MIS-C. However, many children with MIS-C had the virus that causes COVID-19, or had been around someone with COVID-19.”
Laboratory findings in large cohorts of MIS-C have detected varying percentages of SARS-CoV-2 positive PCR tests, and antibodies tests: anywhere from 22% to 56% of children had a positive PCR test, and anywhere between 44% and 99% had detectable SARS-CoV-2 antibodies (Table 2b).
That research paper writes:
It is currently unknown if MIS-C/A might follow immunization against SARS-CoV-2, but a need exists to define this potential entity for monitoring as an adverse event following immunization (AEFI).
It is not known if the vaccine would or could prevent MIS-C. However, this case report on 6 cases of adult MIS-C in Southern California, 3 of the cases developed MIS-C post COVID vaccination.
There is scientific concern and discussion that COVID vaccines in children may trigger the inflammatory conditions that lead to MIS-C:
This kind of inflammatory risk makes vaccine development particularly challenging in the pediatric population. If the vaccine is able to induce this type of antibody response, then it would potentially place otherwise healthy children at risk of severe outcome following vaccination intended to prevent illness from SARS‐CoV‐2.
An early case report of a 14-year-old who was retrospectively diagnosed with MIS-C, details the boy had a history of constipation and eczema, and his father ulcerative colitis: all autoimmune and signs of prior vaccine induced immune dysfunction.
Around 60% of MIS-C are male, and nearly 80% of cases are Hispanic or non-Hispanic Black.
Clinically, MIS-C is very similar to Kawasaki disease, and some surveillance of MIS-C suggests there may be overlap between the two, and:
“Given the overlapping clinical features of MIS-C and Kawasaki disease and the absence of a diagnostic test for either condition, some patients captured by MIS-C surveillance might have had Kawasaki disease.”
It is estimated that 3,000 cases of Kawasaki disease are diagnosed each year in the United States, which can occur post-infection with a virus or bacteria, post-medication, post-chemical, and post-vaccination.
There are many documented case reports of Kawasaki disease triggered or caused by vaccines:
- Case report of infant presenting with Kawasaki Disease 24 hours after a flu shot.
- A case report of infant developing Kawasaki Disease after a vaccine-strain chickenpox breakthrough infection.
- Case report of infant developing Kawasaki Disease after 4 month vaccinations.
All pediatric cases of MIS-C should detail full immunization histories. According to VAERS, there are 3 adolescent cases of MIS-C post COVID vaccination, as of June 4th.
In the year 2016, approximately 5440 hospitalizations with KD were reported among children under 18 years of age in the US; 3935 of these children were under 5 years of age, for a hospitalization rate of 19.8 per 100,000 children in that age group.
Here’s the hard truth: No one wants either, but vaccination may not prevent either, and may cause both.
Bottom Line: MIS-C is rare, may not be mitigated by vaccination, and we may accumulate evidence to the contrary (which we already have for other vaccines): that vaccination increases risk for MIS-C, since it is based in inflammatory responses, and vaccination causes an inflammatory response. As of June 4, there are two reports of MIS-C in VAERS, post COVID vaccination in adolescents.

8. We Aren’t Supposed To Vaccinate A Child For A Disease They Aren’t Even At Risk For
By definition, treating an “illness” in a perfectly healthy person is Munchausen syndrome by proxy.
We must make a distinction here: vaccinating a young healthy person against a disease they are not at risk for is very different than vaccinating an elderly person who is actually at risk for the disease.
I fully support each person’s right to choose what is best for their body, because each person’s situation is unique. But it’s a slippery slope to cast a wide net and assume everyone needs a drug or an injection because 1% of the population might benefit from it.
Because vaccine makers are immune from all liability, and they have added more and more vaccines to the pediatric vaccine schedule over the last few decades, we should be very discerning about adding another 2-dose vaccine to the schedule for a virus that isn’t even a threat to children.
This isn’t the first time the US has tried to pull this kind of thing.
The CDC vaccine schedule currently recommends giving a hepatitis B vaccine to infants on the first day of life, even though they aren’t at risk for the disease at all. You can decline, please know your rights as a parent.
According to the CDC: Who is at risk for hepatitis B?
Although anyone can get hepatitis B, these people are at greater risk:
- Infants born to infected mothers
- People who inject drugs or share needles, syringes, and other types of drug equipment
- Sex partners of people with hepatitis B
- Men who have sex with men
- People who live with someone who has hepatitis B
- Health-care and public-safety workers exposed to blood on the job
- Hemodialysis patients
NOT ON THE LIST: infants born to uninfected mothers. Newborns born to uninfected mothers aren’t at risk. Period. You know who gets hepatitis B? Middle age men!!
Bottom Line: Vaccination is not a risk-free procedure and it should never be done to one person, to protect another. Vaccine makers are immune from all liability, so the parents assume all liability, and the child bears all risk.
Are you willing to put that unknown risk on your child and take full responsibility for if or when something happens to them?
Are you willing to report every vaccine reaction they may have to VAERS.hhs.gov? Because this is the only way signals can get detected.

9. No Long Term Safety Data / VAERS Reports
The vaccines are so new, there is not enough data to know one way or the other just how safe or not safe these vaccines are.
But even so, there are a lot of issues right out of the gate. First there were the reports of anaphylaxis, which is being estimated to occur at a rate of 2.47 per 10,000 vaccinations, then came the elderly sudden deaths in nursing homes, then came the various reports of blood clots in young women and men. Now we have pericarditis and myocarditis in otherwise healthy young men and women, with a clustering around the second dose, suggesting a causal connection.
None of the vaccines are FDA approved, and the clinical trials will not be completed until 2022 and 2023, so it will be a while before we really know the full impact of these shots.
The Pfizer vaccine just began vaccinating 12+ in the community a few weeks ago. So what we have to go on are either anecdotal reports, or VAERS, the Vaccine Adverse Event Reporting System, which may be as much as one month behind on adding reports. It’s a voluntary system, and a lot of people still don’t know where, how, or that they should report vaccine side effects.
VAERS Reports on Adolescents
Accessing VAERS records, so far for all of 2021, ages 6-17 (no COVID vaccines are licensed in children under 12, and ages 12-15 did not begin until May 12. The report I am pulling on 6/16 is reports as of June 4, so this is essentially people over 16, and then people over 12 beginning mid-May):
There were:
- 955 adverse events that involved hospitalization and ER/Office visit
- 67 of those were life threatening
- 15 resulted in permanent disability
- 8 resulted in death
Historically, fewer than 1 percent of adverse events are typically captured. There may be more now, because it’s a new vaccine, and people are more nervous, but there is also caution against promoting vaccine hesitation, so many events may go unreported still.
Analyzing the data
A closer look at the 8 death reports, 2 are the same girl, Kamrynn from Wisconsin (her story is below), who died of a pulmonary embolism less than 2 weeks after the COVID vaccine.
One is the Colorado 15-year-old who died allegedly died of heart failure two days after the Pfizer vaccine.
One is a 15-year-old girl in New Hampshire, a PICU attending who cared for the patients wrote that she suffered cardiac arrest about 3-4 days after her second Moderna shot. A second report appears to also be for her. She died April 6th, and Moderna is not authorized for her age. She had Trisomy 21, and appears to have been severely mentally and physically disabled.
The remaining 3 deaths are all by suicide. One is descriptive with a range of systemic symptoms from vaccination day to death, that include headache, chills, diarrhea, no appetite, and the narrative “he didn’t feel right.” Suicide ideation was noted in the clinical trial in adolescents.
A closer look at the 67 life threatening events reveal:
- 21 episodes of pericarditis or myocarditis
- 2 cases of Guillain-Barre Syndrome
- 4 cases of seizure episodes
- 2 cases of appendicitis
- 9 cases of anaphylaxis
- 4 cases of blood clots
- 3 cases of MIS-C
- 1 suicide attempt that was interrupted and not successful
- 1 paralyzed from the neck down.
A closer look at the 15 events of permanent disability is captured partially in the images below.


Bottom Line: There is more that we don’t know, than we do at this point, when it comes to the vaccine. VAERS does not capture all adverse reactions to vaccination, thus many go unreported and signals take longer to pick up on.
The vaccines may not prevent infection, and definitely wane, thus children face both the risk from the vaccine and the infinitesimally small risk from the virus.
Re: long haulers, this pre-print paper investigates long haul in children, and finds that:
“A chronic inflammatory process and immune dysfunction may 110 explain why some children develop PASC (post-acute sequelae of SARS-CoV-2 infection).”
One more reason not to mess with children’s immune systems. Most diseases and sequelae come back to inflammatory responses, or dysfunctions in the immune system. What could be causing that??

10. Deaths and Serious Injuries After COVID Vaccination More Common In Young People
This is the biggest reason to me. A medical treatment is not supposed to kill people. We aren’t supposed to sacrifice healthy, young people for a hypothetical reduction in disease.
Our perspective of disease is completely skewed: It’s something we prevent through diet and nutrition, through exercise, through encouraging our detox pathways to work properly.
Health does not, and never has, come from a pill bottle or an injection.
I’m sincerely sorry you have been lied to. But your ignorance is not an excuse to put healthy, young people directly in harm’s way.
These young people deserved better.

Simone Scott
Age: 19
Vaccine: Moderna
Simone Scott was a freshman in college, and got both doses of the Moderna shot, despite feeling unwell after the first dose. Within days of the second dose, Simone experienced frequent nose bleeds, a low-grade fever, sore throat, swollen lymph nodes, and irregular heartbeat. Visiting her student health clinic three times in two weeks, she was misdiagnosed, and eventually taken to the hospital already in heart failure. She underwent a heart transplant, but did not survive a lung infection that came next.

Everest Romney
Age: 17
Vaccine: Pfizer
Everest Romney is a 6’9″ high school basketball player in Utah who got the Pfizer vaccine with his mom. Shortly after he began having neck pain, extreme migraines, swelling, and was diagnosed with several blood clots in his brain. He is currently recovering.
His mother Cherie Romney details their family’s experience here, and shares surprisingly that her husband, who had received the Moderna shot, also developed blood clots in response to the mRNA shot, only his was in the lungs and classified as pulmonary embolism. A few weeks later, he also developed blood clots in his brain.

Kamrynn Thomas
Age: 16
Vaccine: First Dose Pfizer
Kamrynn, who was a staff member at summer camp in Wisconsin, was vaccinated on March 19th and suddenly experienced a pulmonary embolism 9 days later. She later died of complications on March 30th.

Maddie
Age: 12
Vaccine: Pfizer
Maddie is a clinical trial participant, and is mentioned in the adverse events section of the Pfizer Fact Sheet, however the trial investigators used great liberty to deny her reaction to the Pfizer shot has a causal connection.

Benjamin Goodman
Age: 32
Vaccine: Johnson & Johnson
Memorial: Benjamin Goodman was 32 years old, and had no pre-existing medical conditions to explain his reaction. He died suddenly within 24 hours of getting the Johnson & Johnson vaccine Janssen. His official cause of death is heart failure.

Dr. Joshimar Henry
Age: 27
Vaccine: Pfizer
Memorial: The young doctor was very fit, and physically active. And to the shock of all his loved ones, Dr. Henry passed away suddenly and unexpectedly April 3, 2021, from a heart attack.

Sara Stickles
Age: 28
Vaccine: Second Dose Pfizer
Memorial: Just five days after the second dose of the Pfizer COVID-19 vaccine, perfectly healthy 28-year-old health care worker Sara had brain aneurysm. Her twin sister stated that Sara had a bad reaction to the vaccine before dying of a stroke caused by the blood clot.

Desiree Penrod
Age: 25
Vaccine: Janssen Single Shot
Memorial: Desiree Penrod was only 25 years old. She had a pre-existing seizure disorder and according to her Facebook page, she had a seizure on Monday, March 8th, one day before she got the vaccine. She died March 17th.

Haley Link Brinkmeyer
Age: 28
Vaccine: Unknown- only first shot
Memorial: Haley was a perfectly healthy 28-year-old who died at her home two days after getting the COVID vaccine. According to her mother, Haley’s autopsy showed no health issues.











Fantastic compilation of the facts! My sincerest thanks to you for taking the time to share this information with other parents. This may save children’s lives in the process. A beautiful light of truth shining in the dark world of lies.