










Vaccine Studies
Select a Category
Please select a category to utilize the accordion menu. If you do not see a study here that you think I should have, please message me and I’ll add it. Thank you!
2023
Neonatal, Infant, and Under Age Five Vaccine Doses Routinely Given in Developed Nations and Their Association With Mortality Rates. Neil Z. Miller, Gary S. Goldman 2023.
There are statistically significant positive correlations between mortality rates of developed nations and the number of early childhood vaccine doses that are routinely given. Further investigations of the hypotheses generated by this study are recommended to confirm that current vaccination schedules are achieving their intended objectives.
A positive correlation between the number of vaccine doses and IMRs is detectable in the most highly developed nations but attenuated in the background noise of nations with heterogeneous socioeconomic variables that contribute to high rates of infant mortality, such as malnutrition, poverty, and substandard health care.
2021
Our findings show a positive correlation between the number of vaccine doses administered and the percentage of hospitalizations and deaths. Since vaccines are given to millions of infants annually, it is imperative that health authorities have scientific data from synergistic toxicity studies on all combinations of vaccines that infants might receive. Finding ways to increase vaccine safety should be the highest priority.
2020
Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disorders. Brian S Hooker, Neil Z Miller. 2020
In this study, which only allowed for the calculation of unadjusted observational associations, higher ORs were observed within the vaccinated versus unvaccinated group for developmental delays, asthma and ear infections[/su_highlight]. Further study is necessary to understand the full spectrum of health effects associated with childhood vaccination.
2018
Evidence of Increase in Mortality After the Introduction of Diphtheria-Tetanus-Pertussis Vaccine to Children Aged 6-35 Months in Guinea-Bissau: A Time for Reflection? Aaby, Peter, et al. 2018
Although having better nutritional status and being protected against three infections, 6-35 months old DTP-vaccinated children tended to have higher mortality than DTP-unvaccinated children. All studies of the introduction of DTP have found increased overall mortality.
A lowered probability of pregnancy in females in the USA aged 25-29 who received a human papillomavirus vaccine injection. DeLong, Gayle. 2018
Results suggest that females who received the HPV shot were less likely to have ever been pregnant than women in the same age group who did not receive the shot. If 100% of females in this study had received the HPV vaccine, data suggest the number of women having ever conceived would have fallen by 2 million. Further study into the influence of HPV vaccine on fertility is thus warranted.
2017
Childhood vaccine status and correlation with common nonvaccine‐preventable illnesses, Michelle M. Anderson DNP, FNP, 2017.
“Fully immunized group had significantly more ear infections than partial or unimmunized. The unimmunized group had significantly more colds and flu.”
Pilot comparative study on the health of vaccinated and unvaccinated 6- to 12-year-old U.S. children, Anthony Mawson, 2017
“The vaccinated were less likely than the unvaccinated to have been diagnosed with chickenpox and pertussis, but more likely to have been diagnosed with pneumonia, otitis media, allergies and NDD. After adjustment, vaccination, male gender, and preterm birth remained significantly associated with NDD. However, in a final adjusted model with interaction, vaccination but not preterm birth remained associated with NDD, while the interaction of preterm birth and vaccination was associated with a 6.6-fold increased odds of NDD (95% CI: 2.8, 15.5). In conclusion, vaccinated homeschool children were found to have a higher rate of allergies and NDD than unvaccinated homeschool children.”
Three case reports of post immunization and post viral Bullous Pemphigoid: looking for the right trigger. Baroero, et al. 2017
Two of [three cases] developed an eruption of bullous lesions just a few days after vaccination for diphtheria, tetanus, pertussis, poliomyelitis, hepatitis B and Haemophilus influenzae B.
2016
The Allergy Epidemics: 1870–2010. Thomas A.E. Platts-Mills 2016
Since 1990 there has been a remarkable increase in food allergy which has now reached epidemic numbers. Peanut has played a major role in the food epidemic and there is increasing evidence that sensitization to peanut can occur through the skin.
Progressive increase in the recommended immunization of children 1950–2010. The number of injections that children receive in early childhood is a concern for many parents and pediatricians. In addition, several authors have suggested a possible role of these injections in the increase in allergic disease or in food allergy in particular.
History of chickenpox in glioma risk: a report from the glioma international case–control study (GICC). E. Susan Amirian, et al. 2016.
Here, we utilized the GICC data to confirm the previously reported associations between history of chickenpox and glioma risk in one of the largest studies to date on this topic. Using two-stage random-effects restricted maximum likelihood modeling, we found that a positive history of chickenpox was associated with a 21% lower glioma risk, adjusting for age and sex (95% confidence intervals (CI): 0.65–0.96). Furthermore, the protective effect of chickenpox was stronger for high-grade gliomas. Our study provides additional evidence that the observed protective effect of chickenpox against glioma is unlikely to be coincidental.
2013
Who is unlikely to report adverse events after vaccinations to the Vaccine Adverse Event Reporting System (VAERS)? McNeil MM, et al. 2013
The percentage of HCP (Healthcare Providers) aware of VAERS (71%) varied by occupation and primary care practice area. About 37% of HCP had identified at least one AEFI with only 17% of these indicating that they had ever reported to VAERS.
[editors note: 17% OF THE 37% had ever reported to VAERS.]
2012
Causality assessment of adverse events reported to the Vaccine Adverse Event Reporting System (VAERS). Loughlin, Anita M, et al. 2012
Access is possible through SCI-hub: https://doi.org/10.1016/j.vaccine.2012.09.074
Increased Risk of Noninfluenza Respiratory Virus Infections Associated With Receipt of Inactivated Influenza Vaccine. Benjamin J. Cowling, et. al. 2012
“We randomized 115 children to trivalent inactivated influenza vaccine (TIV) or placebo. Over the following 9 months, TIV recipients had an increased risk of virologically-confirmed non-influenza infections (relative risk: 4.40; 95% confidence interval: 1.31-14.8). Being protected against influenza, TIV recipients may lack temporary non-specific immunity that protected against other respiratory viruses.”
2011
“Adverse Events following 12 and 18 Month Vaccinations: a Population-Based, Self-Controlled Case Series Analysis.” Kumanan Wilson, et al. 2011
There are significantly elevated risks of primarily emergency room visits approximately one to two weeks following 12 and 18 month vaccination.
Infant mortality rates regressed against number of vaccine doses routinely given: Is there a biochemical or synergistic toxicity? Neil Z Miller and Gary S Goldman. 2011
“Using the Tukey-Kramer test, statistically significant differences in mean IMRs were found between nations giving 12–14 vaccine doses and those giving 21–23, and 24–26 doses. A closer inspection of correlations between vaccine doses, biochemical or synergistic toxicity, and IMRs is essential.”
2006
Frequency of allergic diseases following measles. E. Kucukosmanoglu, et al. 2006.
The results of this study indicate that findings of allergic disease are less frequent in children with a history of measles.
2005
“The relationship between vaccine refusal and self-report of atopic disease in children”. Rachel Enriquez, PhD. 2005
“Parents who refuse vaccinations reported less asthma and allergies in their unvaccinated children.”
2004
Asthma and vaccination history in a young adult cohort. G. Benke, M. Abramson. 2004
However, subjects reporting full immunisation were found to be at higher risk to asthma (RR 1.52, 95% CI 1.09-2.11) but not atopy. Conclusions: Our results show relatively weak support for the hypothesis that childhood vaccinations may lead to increased risk of asthma, but caution is advised due to possible recall bias.
“Vaccination and Allergic Disease: A Birth Cohort Study” Tricia M. McKeever, PhD, 2004.
“Our univariate analysis showed that exposure to DPPT was associated with an increased risk of developing asthma (hazard ratio [HR] = 14.0; 95% confidence interval [CI] = 7.3, 26.9) and eczema (HR = 9.40; 95% CI = 5.92, 14.92)”
In this observational study analyzing computerized primary care records, we found an association between MMR and DPPT vaccination and the incidence of asthma and eczema, but these associations appeared to be limited to the minority of children who rarely seek care from a GP. This limited association is more likely to be the result of bias than a biological effect.”
[Editor’s Note: when an association is found between vaccination and allergy, it is considered bias, because they are so healthy, because they are unvaccinated, that they do not need to see a doctor.]
1992
Symptoms after accelerated immunisation. Mary E B Ramsay, 1992.
[Editor’s note: Out of 107 infants, had reactions to vaccines that compelled the parents to not continue with the pertussis component of the vaccine:
“Only one of the children had a genuine contraindication to further doses of pertussis vaccine, when he developed a temperature of 40.5°C (104.9 degrees F) on evening 2 after vaccination (measured by the mother). The second child was afebrile but seemed distressed with a high pitched cry on the first evening. Although the crying was neither prolonged nor inconsolable and therefore did not constitute a contraindication to further pertussis vaccine, the mother opted to complete with diphtheria-tetanus only vaccine.”
[Editor’s note: We are told that vaccine reactions are “one in a million” and in this study of 107 infants, 2 reportedly had reactions that warranted caution, and exempted at least one of the infants from further vaccination.]
Confounding in Studies of Adverse Reactions to Vaccines, Paul Fine, 1992.
Most published studies have reported a deficit of sudden infant death syndrome among vaccinees, which may reflect confounding in their study designs. An expression is derived to explore the extent of underestimation that may be introduced in such studies, under different sets of conditions. Confounding of this sort is a general problem for studies of adverse reactions to prophylactic interventions, as they may be withheld from some individuals precisely because they are already at high risk of the adverse event.
1991
Evidence Concerning Pertussis Vaccines and Central Nervous System Disorders, Including Infantile Spasms, Hypsarrhythmia, Aseptic Meningitis, and Encephalopathy, Institute of Medicine (US) Committee to Review the Adverse Consequences of Pertussis and Rubella Vaccines; Howson CP. 1991
The evidence is consistent with a causal relation between DPT vaccine and acute encephalopathy,3 defined in the controlled studies reviewed as encephalopathy, encephalitis, or encephalomyelitis.
1989
Anemia of a mild viral infection: the measles vaccine as a model. Olivares M. 1989.
93 infants were immunized with live attenuated measles virus and studied prospectively at 0, 4, 9, 14, 21, and 30 days. Hemoglobin concentration decreased significantly by days 9 and 14. The decrease was greater than 1.0 g/dL in 8.6% and greater than 0.6 in 24.3% of the infants. Of the nonanemic infants, 22% became anemic.
2023
Association Between Aluminum Exposure From Vaccines Before Age 24 Months and Persistent Asthma at Age 24 to 59 Months. Daley, et al.
In a large observational study, a positive association was found between vaccine-related aluminum exposure and persistent asthma. While recognizing the small effect sizes identified and the potential for residual confounding, additional investigation of this hypothesis appears warranted.
2021
“The measurement and full statistical analysis including Bayesian methods of the aluminium content of infant vaccines”. Emma Shardlo, Christopher Exley. 2021
We found that only three vaccines contained the amount of aluminium indicated by the manufacturer. Six vaccines contained a statistically significant (P < 0.05) greater quantity while four vaccines contained a statistically significant (P < 0.05) lower quantity. The range of content for any single vaccine varied considerably, for example, from 0.172 to 0.602 mg/vaccine for Havrix.
2020
“Macrophagic myofasciitis and subcutaneous pseudolymphoma caused by aluminium adjuvants”. Kim, Hyunhee, et al. 2020
Seven child patients with biopsy-proven MMF were retrieved from the Seoul National University Hospital (SNUH) pathology archives from 2015 to 2019.
“Neurotoxic effects of combined exposures to aluminum and mercury in early life (infancy)”. José G Dórea 2020
In the infant (up to six months) the organic-Hg and Al body burdens from a full TCV schedule are estimated to reach levels higher than that originating from breastfeeding or from high aluminum soy-based formulas. Despite worldwide exposure to both Al and Hg (inorganic Hg, MeHg, and Thimerosal/EtHg), our knowledge on this combined exposure is insufficient to predict their combined neurotoxic effects (and with other co-occurring neurotoxicants).
2019
Oral exposure to aluminum leads to reduced nicotinic acetylcholine receptor gene expression, severe neurodegeneration and impaired hippocampus dependent learning in mice. Mehpara Farhat S, et al. 2019
Aluminum (Al) is known for its neurotoxicity for over a century and is reported to have specifically high toxicity for cholinergic system… These results demonstrated that Al exposure caused neurotoxicity in mice hippocampus which is manifested by reduced memory and elevated anxiety. The results were further validated by high Al accumulation in the hippocampus, severe neurodegeneration and reduced expression of nAChRs.
Toxic metals in cord blood and later development of Type 1 diabetes 2019
However, children who later developed T1D had more often increased concentrations (above limit of detection; LOD) of aluminium (p = 0.006) in cord blood than the non-diabetic controls, and also more often mercury and arsenic (n.s).
2018
“Aluminium in brain tissue in autism”. Mold M, Umar D, King A, Exley C. 2018
“The pre-eminence of intracellular aluminium associated with non-neuronal cells was a standout observation in autism brain tissue and may offer clues as to both the origin of the brain aluminium as well as a putative role in autism spectrum disorder.”
Aluminium in Brain Tissue in Multiple Sclerosis. Matthew Mold, et al. 2018
The aluminium content of brain tissue in MS was universally high with many tissues bearing concentrations in excess of 10 μg/g dry wt. (10 ppm) and some exceeding 50 ppm. The association of aluminium with corpora amylacea suggests a role for aluminium in neurodegeneration in MS.
Synergism in aluminum and mercury neurotoxicity. Peter N Alexandrov, Aileen I Pogue. 2018
“This is the first report on the neurotoxic effects of aluminum sulfate and/or mercury sulfate on the initiation of inflammatory signaling in human brain cells in primary culture. The effects aluminum+mercury together on other neurologically important signaling molecules or the effects of other combinations of common environmental metallic neurotoxins to human neurobiology currently remain not well understood but certainly warrant additional investigation and further study in laboratory animals, in human primary tissue cultures of CNS cells, and in other neurobiologically realistic experimental test systems.”
2017
“Non-linear dose-response of aluminium hydroxide adjuvant particles: Selective low dose neurotoxicity”. Crépeaux G, et. al. 2017
An unusual neuro-toxicological pattern limited to a low dose of Alhydrogel® was observed. Neurobehavioural changes, including decreased activity levels and altered anxiety-like behaviour, were observed compared to controls in animals exposed to 200μg Al/kg but not at 400 and 800μg Al/kg…..We conclude that Alhydrogel® injected at low dose in mouse muscle may selectively induce long-term Al cerebral accumulation and neurotoxic effects.
“The putative role of environmental aluminium in the development of chronic neuropathology in adults and children. How strong is the evidence and what could be the mechanisms involved?”. Gerwyn Morris, Basant K. Puri, and Richard E. Frye. 2017
2016
“Aluminum in Childhood Vaccines Is Unsafe” Neil Z. Miller. 2016
Aluminum is a neurotoxin, yet infants and young children are repeatedly injected with aluminum adjuvants from multiple vaccines during critical periods of brain development. Numerous studies provide credible evidence that aluminum adversely affects important biological functions and may contribute to neurodegenerative and autoimmune disorders. It is impossible to predetermine which vaccinated babies will succumb to aluminum poisoning. Aluminum-free health options are needed.
2015
“Exposure to Mercury and Aluminum in Early Life: Developmental Vulnerability as a Modifying Factor in Neurologic and Immunologic Effects.” José G. Dórea. 2015
“Currently, ethylmercury (EtHg) and adjuvant-Al are the dominating interventional exposures encountered by fetuses, newborns, and infants due to immunization with Thimerosal-containing vaccines (TCVs). Despite their long use as active agents of medicines and fungicides, the safety levels of these substances have never been determined, either for animals or for adult humans—much less for fetuses, newborns, infants, and children……More research attention has been given to EtHg and findings have showed a solid link with neurotoxic effects in humans; however, the potential synergic effect of both toxic agents has not been properly studied. Therefore, early life exposure to both EtHg and Al deserves due consideration.”
In univariable General Linear Models, the geometric mean cord blood aluminum concentration was higher for children whose mothers had completed their education up to high school compared to those whose mothers had any education beyond high school (12.2 μg/L vs. 6.4 μg/L; p < 0.01)
2013
“Effect of Routine Vaccination on Aluminum and Essential Element Levels in Preterm Infants.” Tammy Z. Movsas 2013
No significant change in levels of urinary or serum aluminum were seen after vaccination. Significant declines were noted postvaccination in serum iron (58.1%), manganese (25.9%), selenium (9.5%), and zinc (36.4%) levels, as was a significant increase in serum copper level (8.0%). A rise in selenium level was the only significant urine change.
[Editor’s note: An increase in post-vaccination serum or urine levels of Aluminum was not detected because Aluminum adjuvants are not quickly excreted, which lends further support to the hypothesis that Aluminum adjuvants bioaccumulate and translocate to other parts of the body, for example, the brain.]
“Mechanisms of aluminum adjuvant toxicity and autoimmunity in pediatric populations”. Tomljenovic L, Shaw CA. 2012
“Autoimmunity following hepatitis B vaccine as part of the spectrum of ‘Autoimmune (Auto-inflammatory) Syndrome induced by Adjuvants’ (ASIA): analysis of 93 cases”. Zafrir Y, Agmon-Levin N, Paz Z, Shilton T, Shoenfeld Y. 2012
Aluminum Adjuvant Linked to Gulf War Illness Induces Motor Neuron Death in Mice, Michael S. Petrik. 2007.
The findings suggest a possible role for the aluminum adjuvant in some neurological features associated with GWI and possibly an additional role for the combination of adjuvants.
2021
“Preterm or Early Term Birth and Risk of Autism.” Casey Crumb. et al. 2021
“Reviewing the association between aluminum adjuvants in the vaccines and autism spectrum disorder“Alberto Boretti. 2021
The association between aluminum adjuvants in the vaccines and autism spectrum disorder is suggested by multiple lines of evidence.
2018
Aluminium in brain tissue in autism. Matthew Mold, Dorcas Umar, Andrew King, Christopher Exley. 2018
“While aluminium was imaged associated with neurones it appeared to be present intracellularly in microglia-like cells and other inflammatory non-neuronal cells in the meninges, vasculature, grey and white matter. The pre-eminence of intracellular aluminium associated with nonneuronal cells was a standout observation in autism brain tissue and may offer clues as to both the origin of the brain aluminium as well as a putative role in autism spectrum disorder.
“Immunoexcitotoxicity as the central mechanism of etiopathology and treatment of autism spectrum disorders: A possible role of fluoride and aluminum” Anna Strunecka, Russell L. Blaylock, Jiri Patocka, and Otakar Strunecky. 2018
“We demonstrate that fluoride and aluminum (Al3+) can exacerbate the pathological problems by worsening excitotoxicity and inflammation. While Al3+ appears among the key suspicious factors of ASD, fluoride is rarely recognized as a causative culprit. A long-term burden of these ubiquitous toxins has several health effects with a striking resemblance to the symptoms of ASD.”
“Premature Puberty and Thimerosal-Containing Hepatitis B Vaccination: A Case-Control Study in the Vaccine Safety Datalink.” Geier, et al. 2018
“The results of this study show a dose-dependent association between increasing organic Hg exposure from Thimerosal-containing hepatitis B vaccines administered within the first six months of life and the long-term risk of the child being diagnosed with premature puberty.”
2017
Association Between Influenza Infection and Vaccination During Pregnancy and Risk of Autism Spectrum Disorder. Ousseny Zerbo, PhD, et al. 2017
In trimester-specific analyses, first-trimester influenza vaccination was the only period associated with increased ASD risk (adjusted hazard ratio, 1.20; 95% CI, 1.04-1.39). However, this association could be due to chance.
Maternal breastfeeding and autism spectrum disorder in children: A systematic review and meta-analysis. Tseng PT 2017
This meta-analysis provides evidence that breastfeeding (exclusively or including additional supplements) may protect against ASD. Prospective longitudinal research is required to disentangle the complex relationships and to explore potential pathophysiological mechanisms.
2014
“Vaccines are not associated with autism: An evidence-based meta-analysis of case-control and cohort studies” Luke E. Taylor, Amy L. Swerdfeger, Guy D. Eslick. 2014
“Studies were included that looked at either MMR vaccination, cumulative mercury (Hg) or cumulative thimerosal dosage from vaccinations to ensure all proposed causes of ASD or regression were investigated.”
[Editor’s note: Please take special note that only MMR vaccine, and or cumulative mercury exposure, was investigated before coming to the conclusion that ALL VACCINES are not associated with Autism. Please see further articles here.]
“Transcriptomic analyses of neurotoxic effects in mouse brain after intermittent neonatal administration of thimerosal.” Li X,Qu F,Xie W, et al. 2014
“Thimerosal-treated mice exhibited neural development delay, social interaction deficiency, and inclination of depression.”
“Methodological Issues and Evidence of Malfeasance in Research Purporting to Show Thimerosal in Vaccines Is Safe”. Brian Hooker, et al. 2014
2013
Assessment of Infantile Mineral Imbalances in Autism Spectrum Disorders (ASDs). Hiroshi Yasuda and Toyoharu Tsutsui. 2013.
These findings suggest that infantile zinc- and magnesium-deficiency and/or toxic metal burdens may be critical and induce epigenetic alterations in the genes and genetic regulation mechanisms of neurodevelopment in the autistic children, and demonstrate that a time factor “infantile window” is also critical for neurodevelopment and probably for therapy.
“Maternal immune activation causes age and region-specific changes in brain cytokines in offspring throughout development.” Garay, Paula A. Hsiao, Elaine Y. Patterson, Paul H. McAllister, A K. Brain, behavior, and immunity 2013; 31():54-68 PubMed Link
“Together, these data indicate that MIA leads to long-lasting, region-specific changes in brain cytokines in offspring—similar to those reported for ASD and SZ—that may alter CNS development and behavior.”
2012
Toxic Metals and Essential Elements in Hair and Severity of Symptoms among Children with Autism. Eleonor BLAUROCK-BUSCH. 2012
Our data supports the historic evidence that heavy metals play a role in the development of ASD. In combination with an inadequate nutritional status the toxic effect of metals increase along with the severity of symptoms.
2011
“Hypothesis: conjugate vaccines may predispose children to autism spectrum disorders.“ Richmand BJ. Med Hypotheses. 2011.
Conjugate vaccines fundamentally change the manner in which the immune systems of infants and young children function by deviating their immune responses to the targeted carbohydrate antigens from a state of hypo-responsiveness to a robust B2 B cell mediated response. This period of hypo-responsiveness to carbohydrate antigens coincides with the intense myelination process in infants and young children, and conjugate vaccines may have disrupted evolutionary forces that favored early brain development over the need to protect infants and young children from capsular bacteria.
“A positive association found between autism prevalence and childhood vaccination uptake across the U.S. population”. Delong G. 2011
“A positive and statistically significant relationship was found: The higher the proportion of children receiving recommended vaccinations, the higher was the prevalence of AUT or SLI. A 1% increase in vaccination was associated with an additional 680 children having AUT or SLI.”
2009
“Hepatitis B vaccination of male neonates and autism diagnosis, NHIS 1997-2002″. Gallagher CM, Goodman MS. 2010
“Findings suggest that U.S. male neonates vaccinated with the hepatitis B vaccine prior to 1999 (from vaccination record) had a threefold higher risk for parental report of autism diagnosis compared to boys not vaccinated as neonates during that same time period.”
2009
“Immune-glutamatergic dysfunction as a central mechanism of the autism spectrum disorders”. Blaylock RL, Strunecka A. 2009
“We suggest that environmental and dietary excitotoxins, mercury, fluoride, and aluminum can exacerbate the pathological and clinical problems by worsening excitotoxicity and by microglial priming.”
“What is regressive autism and why does it occur? Is it the consequence of multi-systemic dysfunction affecting the elimination of heavy metals and the ability to regulate neural temperature?” Graham E. Ewing. 2009
This article explores the issues and concludes that sensory dysfunction and systemic failure, manifested as autism, is the inevitable consequence arising from subtle DNA alteration and consequently from the overuse of vaccines.
2008
“Acetaminophen (paracetamol) use, measles-mumps-rubella vaccination, and autistic disorder: the results of a parent survey.” Schultz ST, et al. 2008
“Acetaminophen use after measles-mumps-rubella vaccination was significantly associated with autistic disorder when considering children 5 years of age or less (OR 6.11, 95% CI 1.42-26.3), after limiting cases to children with regression in development (OR 3.97, 95% CI 1.11-14.3), and when considering only children who had post-vaccination sequelae (OR 8.23, 95% CI 1.56-43.3), adjusting for age, gender, mother’s ethnicity, and the presence of illness concurrent with measles-mumps-rubella vaccination.”
2007
“Maternal Immune Activation Alters Fetal Brain Development through Interleukin-6”. Stephen E. P. Smith, Jennifer Li, Krassimira Garbett, Karoly Mirnics, and Paul H. Patterson. 2007
A prospective study of thimerosal-containing Rho(D)-immune globulin administration as a risk factor for autistic disorders. Geier DA, Geier MR. 2007
“Children with ASDs (28.30%) were significantly more likely (odds ratio 2.35, 95% confidence interval 1.17-4.52, p < 0.01) to have Rh-negative mothers than controls (14.36%). Each ASD patient’s mother was determined to have been administered a TCR during her pregnancy.”
2006
Environmental mercury release, special education rates, and autism disorder: an ecological study of Texas, Raymond F. Palmera, 2006
On average, for each 1000 lb of environmentally released mercury, there was a 43% increase in the rate of special education services and a 61% increase in the rate of autism. The association between environmentally released mercury and special education rates were fully mediated by increased autism rates. This ecological study suggests the need for further research regarding the association between environmentally released mercury and developmental disorders such as autism. These results have implications for policy planning and cost analysis.
Breastfeeding, infant formula supplementation, and Autistic Disorder: the results of a parent survey. Stephen T Schultz 2006
The results of this preliminary study indicate that children who were not breastfed or were fed infant formula without docosahexaenoic acid/arachidonic acid supplementation were significantly more likely to have autistic disorder.
2005
“Immunological findings in autism”. Cohly HH, Panja A. 2005
2003
“Elevated levels of measles antibodies in children with autism”. Singh VK, Jensen RL. 2003
2002
“Abnormal measles-mumps-rubella antibodies and CNS autoimmunity in children with autism”. Singh VK, et al. 2002
1998
“RETRACTED: Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children“ Andrew Wakefield, et al. 1998
“Onset of behavioural symptoms was associated, by the parents, with measles, mumps, and rubella vaccination in eight of the 12 children, with measles infection in one child, and otitis media in another. All 12 children had intestinal abnormalities, ranging from lymphoid nodular hyperplasia to aphthoid ulceration. Histology showed patchy chronic inflammation in the colon in 11 children and reactive ileal lymphoid hyperplasia in seven, but no granulomas. Behavioural disorders included autism (nine), disintegrative psychosis (one), and possible postviral or vaccinal encephalitis (two). There were no focal neurological abnormalities and MRI and EEG tests were normal. Abnormal laboratory results were significantly raised urinary methylmalonic acid compared with agematched controls (p=0·003), low haemoglobin in four children, and a low serum IgA in four children.Interpretation
We identified associated gastrointestinal disease and developmental regression in a group of previously normal children, which was generally associated in time with possible environmental triggers.”
1982
“Abnormal immune response to brain tissue antigen in the syndrome of autism” A Weizman, et al. 1982
“Cell-mediated immune response to human myelin basic protein was studied by the macrophage migration inhibition factor test in 17 autistic patients and a control group of 11 patients suffering from other mental diseases included in the differential diagnosis of the syndrome of autism. Of the 17 autistic patients, 13 demonstrated inhibition of macrophage migration, whereas none of the nonautistic patients showed such a response. The results indicate the existence of a cell-mediated immune response to brain tissue in the syndrome of autism.”
1976
“[Autistic syndrome (Kanner) and vaccination against smallpox (author’s transl)]” C Eggars. 1976
“3-4 weeks following an otherwise uncomplicated first vaccination against smallpox a boy, then aged 15 months and last seen at the age of 5 1/2 years, gradually developed a complete Kanner syndrome. The question whether vaccination and early infantile autism might be connected is being discussed. A causal relationship is considered extremely unlikely. But vaccination is recognized as having a starter function for the onset of autism.”
Severe Herpes Zoster Following Varicella Vaccination in Immunocompetent Young Children. Moodley A 2019.
Since varicella vaccine is a live attenuated virus, the virus replicates in the skin after administration and can travel via sensory nerves or viremia to become latent in the dorsal root ganglia. In some immunized children, virus reactivates within a few months to a few years to cause the dermatomal exanthem known as herpes zoster (shingles).
One of the children with herpes zoster subsequently developed asthma, a known risk factor for herpes zoster, but none of the children had an autoimmune disease. Although postherpetic neuralgia is exceedingly rare, children who develop herpes zoster following varicella vaccination are at risk (albeit low) of developing meningoencephalitis and should be carefully observed for a few weeks.
Neonatal varicella: Probable transmission from a vaccinated mother. Hajime Machi, et al. 2018.
History of chickenpox in glioma risk: a report from the glioma international case–control study (GICC). E. Susan Amirian, et al. 2016.
Here, we utilized the GICC data to confirm the previously reported associations between history of chickenpox and glioma risk in one of the largest studies to date on this topic. Using two-stage random-effects restricted maximum likelihood modeling, we found that a positive history of chickenpox was associated with a 21% lower glioma risk, adjusting for age and sex (95% confidence intervals (CI): 0.65–0.96). Furthermore, the protective effect of chickenpox was stronger for high-grade gliomas. Our study provides additional evidence that the observed protective effect of chickenpox against glioma is unlikely to be coincidental.
Transmission of varicella vaccine virus to a non-family member in China. Lin Gan, et al. 2011.
Transmission of varicella-vaccine virus from a healthy 12-month-old child to his pregnant mother. Salzman MB, et al. 1997
A 12-month-old healthy boy had approximately 30 vesicular skin lesions 24 days after receiving varicella vaccine. Sixteen days later his pregnant mother had 100 lesions. Varicella-vaccine virus was identified by polymerase chain reaction in the vesicular lesions of the mother. After an elective abortion, no virus was detected in the fetal tissue. This case documents transmission of varicella-vaccine virus from a healthy 12-month-old infant to his pregnant mother.
Ivermectin Prophylaxis Used for COVID-19: A Citywide, Prospective, Observational Study of 223,128 Subjects Using Propensity Score Matching. 2022. Link Here.
The regular use of ivermectin led to a 68% reduction in COVID-19 mortality (25 [0.8%] versus 79 [2.6%] among ivermectin non-users; RR, 0.32; 95% CI, 0.20-0.49; p < 0.0001).
The mechanisms of action of Ivermectin against SARS-CoV-2: An evidence-based clinical review article. 2021 https://www.nature.com/articles/s41429-021-00430-5#Tab1
Random effects meta-analysis with pooled effects showed 79% improvement for early treatment RR 0.21 and CI [0.11-0.37]
Random effects meta-analysis with pooled effects showed 46% improvement for late treatment RR 0.54 and CI [0.40-0.72]
The effect of early treatment with ivermectin on viral load, symptoms and humoral response in patients with non-severe COVID-19: A pilot, double-blind, placebo-controlled, randomized clinical trial. 2021 https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(20)30464-8/fulltext
Among patients with non-severe COVID-19 and no risk factors for severe disease receiving a single 400 mcg/kg dose of ivermectin within 72 h of fever or cough onset there was no difference in the proportion of PCR positives. There was however a marked reduction of self-reported anosmia/hyposmia, a reduction of cough and a tendency to lower viral loads and lower IgG titers which warrants assessment in larger trials.
Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19) 2020 https://rcm.imrpress.com/article/2020/2153-8174/RCM2020264.shtml
Prompt early initiation of sequenced multidrug therapy (SMDT) is a widely and currently available solution to stem the tide of hospitalizations and death. A multipronged therapeutic approach includes 1) adjuvant nutraceuticals, 2) combination intracellular anti-infective therapy, 3) inhaled/oral corticosteroids, 4) antiplatelet agents/anticoagulants, 5) supportive care including supplemental oxygen, monitoring, and telemedicine.
Use of Ivermectin Is Associated With Lower Mortality in Hospitalized Patients With Coronavirus Disease 2019. 2021 https://journal.chestnet.org/article/S0012-3692(20)34898-4/fulltext
Ivermectin treatment was associated with lower mortality during treatment of COVID-19, especially in patients with severe pulmonary involvement.
The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. June 2020 https://www.sciencedirect.com/science/article/pii/S0166354220302011
We report here that Ivermectin, an FDA-approved anti-parasitic previously shown to have broad-spectrum anti-viral activity in vitro, is an inhibitor of the causative virus (SARS-CoV-2), with a single addition to Vero-hSLAM cells 2 h post infection with SARS-CoV-2 able to effect ~5000-fold reduction in viral RNA at 48 h. Ivermectin therefore warrants further investigation for possible benefits in humans.
Impact of Serum 25(OH) Vitamin D Level on Mortality in Patients with COVID-19 in Turkey October 2020 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7533663/
Vitamin D insufficiency was present in 93.1% of the patients with severe-critical COVID-19.Serum 25(OH) vitamin D was independently associated with mortality in COVID-19 patients.
The impact of vitamin D supplementation on mortality rate and clinical outcomes of COVID-19 patients: A systematic review and meta-analysis. Jan. 2021. https://www.medrxiv.org/content/10.1101/2021.01.04.21249219v1
Prescribing vitamin D supplementation to patients with COVID-19 infection seems to decrease the mortality rate, the severity of the disease, and serum levels of the inflammatory markers.
Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. November 2020. https://www.nature.com/articles/s41598-020-77093-z
The prevalence of vitamin D deficiency was 32.96% and 96.82% respectively in Group A (asymptomatic patients) and Group B (critically ill patients). Out of total 154 patients, 90 patients were found to be deficient in vitamin D.
Vitamin D level is markedly low in severe COVID-19 patients. Inflammatory response is high in vitamin D deficient COVID-19 patients. This all translates into increased mortality in vitamin D deficient COVID-19 patients. As per the flexible approach in the current COVID-19 pandemic authors recommend mass administration of vitamin D supplements to population at risk for COVID-19.
Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. Sept. 2020. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0239799
Six Month Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. July 2021 PREPRINT
During the blinded, controlled period, 15 BNT162b2 and 14 placebo recipients died; during the open-label period, 3 BNT162b2 and 2 original placebo recipients who received BNT162b2 after unblinding died. None of these deaths were considered related to BNT162b2 by investigators. Causes of death were balanced between BNT162b2 and placebo groups (Table S4).
Israeli public health data slide show. Reduced efficacy over 7 months.
Increased risks of haematological and vascular events that led to hospital admission or death were observed for short time intervals after first doses of the ChAdOx1 nCoV-19 and BNT162b2 mRNA vaccines. The risks of most of these events were substantially higher and more prolonged after SARS-CoV-2 infection than after vaccination in the same population.
Obesity may hamper SARS-CoV-2 vaccine immunogenicity. Feb 2021. https://www.scribd.com/document/497798033/OBESITY-MAY-HAMPER-SARS-CoV-2-VACCINE-IMMUNOGENICITY
“These findings imply that females, lean and young people have an increased capacity to mount humoral immune responses compared to males, overweight and the older population.”
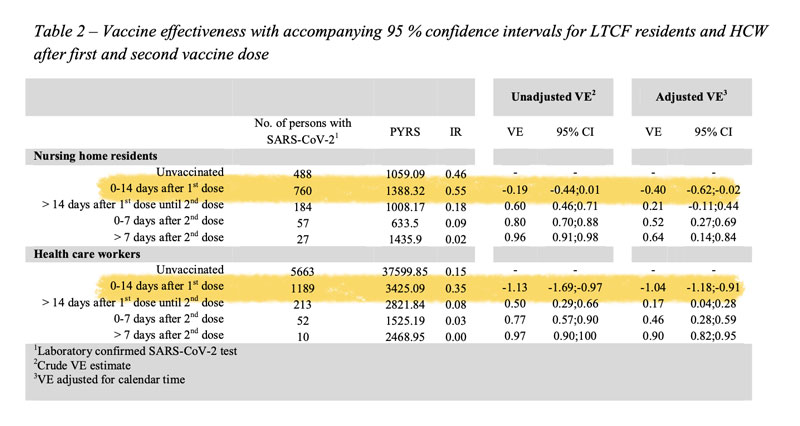
“Vaccine effectiveness after 1st and 2nd dose of the BNT162b2 mRNA Covid-19 Vaccine in long-term care facility residents and healthcare workers – a Danish cohort study” 2021 https://www.medrxiv.org/content/medrxiv/early/2021/03/09/2021.03.08.21252200.full.pdf
Results: No protective effect was observed for LTCF residents after first dose.
According to the table in the study, both health care workers and nursing home patients experienced higher incidence of covid cases compared to unvaccinated, 40% higher and 100% higher in nursing home residents, and health care workers.
BMJ Letter Rapid Response Re: previous study: “Why don’t Covid-19 vaccine trials report statistics for the first 14 days?” Allan S. Cunningham. 2021 https://www.bmj.com/content/372/bmj.n728/rr-0
Recently a pediatric colleague sent me this preprint link to a Danish cohort study of the Pfizer Covid-19 vaccine in long-term care facility residents and healthcare workers. (https://www.medrxiv.org/content/10.1101/2021.03.08.21252200v1 ) It showed real-world effectiveness of two doses of the mRNA vaccine: 64% and 90% VE in the two groups respectively beyond seven days after the second dose.
However, from 0 to 14 days after the first dose the risk of Covid-19 infection was actually increased in vaccine recipients: in the LTCF residents VE was -40%, CI -62% to -2%; among healthcare workers VE was -104%, CI -118% to -91%.(Table 2)…..By contrast, statistics for the 0 to 14 days after the first dose were not reported in the randomized trials of the Pfizer, Moderna, or AstraZeneca vaccines. (Polack et al, NEJM 2020;383:2603. Baden et al, NEJM 2021;384:403. Voysel et al, Lancet 2021;397:92) Why not? Are the manufacturers hiding negative data?
BMJ Letter Rapid Response: “Will covid-19 vaccines save lives? Current trials aren’t designed to tell us” Indrani Roy 2021 https://www.bmj.com/content/371/bmj.m4037/rr-20
“Here I would like to bring attention to an urgent and very important issue of its indirect effect. Apart from the direct side effect after vaccination, if any; the secondary effect that might be caused due to mutation of the virus after mass vaccination needs attention too.
For Brazil, vaccination started in mid-January and a sharp rise in cases is observed since mid-February. Such a steep rise in deaths in Brazil that happened for the last one month never happened in the whole period of pandemic. It already reached twice the height of previous peaks [3]. Globally, the cases started increasing after 5 weeks of a steady decline and coincidentally, the period of rise matches when major vaccination programmes were initiated worldwide.”
Estimating the effectiveness of the Pfizer COVID-19 BNT162b2 vaccine after a single dose. A reanalysis of a study of ‘real-world’ vaccination outcomes from Israel. Feb. 2021. https://www.medrxiv.org/content/medrxiv/early/2021/02/03/2021.02.01.21250957.full.pdf
“After initial injection case numbers increased to day 8 before declining to low levels by day 21. Estimated vaccine effectiveness was pretty much 0 at day 14 but then rose to about 90% at day 21 before levelling off.”
Evidence of Increase in Mortality After the Introduction of Diphtheria-Tetanus-Pertussis Vaccine to Children Aged 6-35 Months in Guinea-Bissau: A Time for Reflection? Aaby, Peter, et al. 2018
Although having better nutritional status and being protected against three infections, 6-35 months old DTP-vaccinated children tended to have higher mortality than DTP-unvaccinated children. All studies of the introduction of DTP have found increased overall mortality.
“Prenatal Tdap immunization and risk of maternal and newborn adverse events” J Bradley Layton, 2017
The risks of many birth outcomes were similar between those who did and did not receive Tdap during pregnancy (see Table 3). However, optimally-timed Tdap was associated with a small increase in chorioamnionitis [IPTW-weighted risks: 3.3% optimally immunized women, 3.0% unimmunized women; RR=1.11 (95% CI: 1.07–1.15)] and post-partum hemorrhage [IPTW-weighted risks: 2.9% optimally immunized women, 2.4% unimmunized women; RR=1.23 (95% CI: 1.18–1.28), as compared to women who did not receive Tdap during pregnancy. Early Tdap receipt was also associated with chorioamnionitis [IPTW-weighted risks: 3.6% in early immunized women, 2.8% in unimmunized women; RR=1.19 (95% CI: 1.11–1.28)], and post-partum hemorrhage, [IPTW-weighted risks: 3.13% early immunized women, 2.3% unimmunized women; RR=1.34 (95% CI: 1.25–1.44)], and additionally with premature rupture of membranes [IPTW-weighted risks: 5.2% in early immunized women, 4.9% in unimmunized women; RR=1.08 (95% CI: 1.02–1.15)]
The Introduction of Diphtheria-Tetanus-Pertussis and Oral Polio Vaccine Among Young Infants in an Urban African Community: A Natural Experiment. Mogensen, et al. 2017
Results: Among 3–5-month-old children, having received DTP (±OPV) was associated with a mortality hazard ratio (HR) of 5.00 (95% CI 1.53–16.3) compared with not-yet-DTP-vaccinated children. Differences in background factors did not explain the effect. The negative effect was particularly strong for children who had received DTPonly and no OPV (HR = 10.0 (2.61–38.6)). All-cause infant mortality after 3 months of age increased after the introduction of these vaccines (HR = 2.12 (1.07–4.19)).
Asymptomatic transmission and the resurgence of Bordetella pertussis. Benjamin M. Althouse. 2015
Although a clear role for the previously suggested mechanisms still exists, asymptomatic transmission is the most parsimonious explanation for many of the observations surrounding the resurgence of B. pertussis in the US and UK.
Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model. Jason M. Warfel, et al. 2013
Baboons vaccinated with aP were protected from severe pertussis-associated symptoms but not from colonization, did not clear the infection faster than naïve animals, and readily transmitted B. pertussis to unvaccinated contacts.
Anti-NMDA receptor encephalitis after TdaP–IPV booster vaccination: cause or coincidence? Caroline Hofmann, et al. 2011.
We report about a 15-year-old female patient who was diagnosed with anti-NMDA receptor encephalitis after receiving a booster vaccination against tetanus/diphtheria/ pertussis and polio (TdaP-IPV).
Delay in diphtheria, pertussis, tetanus vaccination is associated with a reduced risk of childhood asthma. Kara L. McDonald, MSc, et al. 2008.
We found a negative association between delay in administration of the first dose of whole-cell DPT immunization in childhood and the development of asthma; the association was greater with delays in all of the first 3 doses. The mechanism for this phenomenon requires further research.
“Deaths related to the injection of foreign protein in man are fortunately few. The exact number of such occurrences is difficult to estimate from the available literature. By 1942 Kojis1 was able to find 61 such deaths, and he added 4 more from the Willard Parker Hospital. The most complete and most recent study of necropsies was made by Vance and Strassmann,2 who added 7 autopsy studies from the Office of the Chief Medical Examiner to 19 taken from the literature. Park3 in 1932 recorded the mortality from serum anaphylaxis as 0.002 per cent. Kojis1 in 1942 found it to be just under 0.1 per cent in a series of 6,211 subjects treated for various infections. Rutstein and his associates,4 in their analysis of pneumonia cases treated with antipneumococcus horse serum, found the mortality to be 0.45 per cent.”
Cervical intraepithelial neoplasia grade 3 in a patient following Gardasil vaccination. Bruce McLucas, et al. 2019
A 33-year-old woman (Gravida 2, Para 2) received Gardasil in 2006. Subsequently, her pap smear revealed low grade squamous intraepithelial lesion. Cervical biopsies performed in 2015 and 2016 revealed cervical intraepithelial neoplasia grade 1 (CIN 1). She underwent loop electrosurgical excision procedure for persistent CIN 1, which demonstrated CIN 3.
Human papilloma virus-associated squamous cell carcinoma of the larynx in an 18-year-old woman. Hotz MA, et al. 2019
Benign lesion appearance and quadrivalent HPV vaccine status do not exclude HPV-associated malignancies. In our patient, the Gardasil vaccine did not provide crossover protection against HPV 45 infection.
A lowered probability of pregnancy in females in the USA aged 25–29 who received a human papillomavirus vaccine injection. Gayle DeLong. 2018.
Shortly after the vaccine was licensed, several reports of recipients experiencing primary ovarian failure emerged. This study analyzed information gathered in National Health and Nutrition Examination Survey, which represented 8 million 25-to-29-year-old women residing in the United States between 2007 and 2014. Approximately 60% of women who did not receive the HPV vaccine had been pregnant at least once, whereas only 35% of women who were exposed to the vaccine had conceived.
Myasthenia gravis following human papillomavirus vaccination: a case report. Chung JY, et al. 2018
A 23-year-old woman presented with binocular diplopia, ptosis, dysarthria, and dysphagia, which occurred on the 3rd day after the second HPV vaccine administration. She was diagnosed with MG based on history, clinical features, and test results. Her symptoms deteriorated on the 3rd day after admission, and she was transferred to the intensive care unit with mechanical ventilation.
HPV vaccination may cause MG owing to unexpected abnormal autoimmune responses. Additional studies are needed to clarify the possible causal relationship between the HPV vaccine and neurological complications and to evaluate the safety of the vaccine.
Adolescent Premature Ovarian Insufficiency Following Human Papillomavirus Vaccination. Little, et al. 2014
Three young women who developed premature ovarian insufficiency following quadrivalent human papillomavirus (HPV) vaccination presented to a general practitioner in rural New South Wales, Australia. The unrelated girls were aged 16, 16, and 18 years at diagnosis. Each had received HPV vaccinations prior to the onset of ovarian decline.
Human papilloma virus vaccine and primary ovarian failure: another facet of the autoimmune/inflammatory syndrome induced by adjuvants. Colafrancesco S, et al. 2013
We documented here the evidence of the potential of the HPV vaccine to trigger a life-disabling autoimmune condition. The increasing number of similar reports of post HPV vaccine-linked autoimmunity and the uncertainty of long-term clinical benefits of HPV vaccination are a matter of public health that warrants further rigorous inquiry.
Detection of human papillomavirus L1 gene DNA fragments in postmortem blood and spleen after Gardasil® vaccination—A case report. Sin Hang Lee. 2012
A same-nested PCR was used to re-amplify the amplicon of a hypervariable region of the HPV-16 L1 gene DNA in the postmortem blood and splenic tissue obtained at autopsy of a formerly healthy teenage girl who suffered a sudden unexpected death in sleep 6 months after 3 intramuscular injections of a quadrivalent HPV vaccine, Gardasil®. A full autopsy analysis revealed no cause of death.
These naked non-proliferating HPV16 L1 gene DNA fragments appeared to be in the macrophages of the postmortem blood and spleen, and were protected from degradation by binding firmly to the particulate aluminum adjuvant used in vaccine formulation. The significance of these HPV DNA fragments of a vaccine origin found in postmortem materials is not clear and warrants further investigation.
Anaphylaxis following quadrivalent human papillomavirus vaccination. Julia M.L. Brotherton, et al. 2008
From the 269,680 HPV vaccine doses administered in schools, 7 cases of anaphylaxis were identified, which represents an incidence rate of 2.6 per 100 000 doses (95% CI 1.0–5.3 per 100 000). In comparison, the rate of identified anaphylaxis was 0.1 per 100 000 doses (95% CI 0.003–0.7) for conjugated meningococcal C vaccination in a 2003 school-based program.
Based on the number of confirmed cases, the estimated rate of anaphylaxis following quadrivalent HPV vaccine was significantly higher than identified in comparable school-based delivery of other vaccines.
Inflammatory Arthritis following Hepatitis B Vaccination in an Infant. Sana S. Rahimi. 2021
“Herein, we describe the first reported case of an infant who developed inflammatory arthritis following hepatitis B vaccination. A 10-day-old female presented for evaluation of decreased movement of the right lower extremity and right knee swelling. Of note, the patient received a hepatitis B vaccine in her right thigh at birth. A workup found the patient to have a negative ANA but the presence of HLA B27.”
Premature Puberty and Thimerosal-Containing Hepatitis B Vaccination: A Case-Control Study in the Vaccine Safety Datalink. Geier, et al. 2018
The results of this study show a dose-dependent association between increasing organic Hg exposure from Thimerosal-containing hepatitis B vaccines administered within the first six months of life and the long-term risk of the child being diagnosed with premature puberty.
Hepatitis B vaccination of male neonates and autism diagnosis, NHIS 1997-2002. Gallagher, et al. 2010.
Findings suggest that U.S. male neonates vaccinated with thehepatitis B vaccineprior to 1999 (from vaccination record) had a threefold higher risk for parental report of autism diagnosis compared to boys not vaccinated as neonates during that same time period. Nonwhite boys bore a greater risk.
An investigation of infant deaths following initial hepatitis B vaccination based on the Vaccine Adverse Event Reporting System (VAERS), 1992-2002. Soldatenkova, et al. 2007
“In most of the reviewed cases, the history, the symptoms and or the pathologic findings did not support the classification of death as unexplained or SIDS. All cases of “SIDS” occurring shortly after vaccination should be reported to VAERS.
The risks of vaccinating premature, small or slightly ill infants should be weighed against the benefits of each vaccine, particularly in cases where the vaccine is not even needed.
The role of low serum ascorbate in SIDS should be further investigated particularly since the number of recommended pediatric vaccines is constantly increasing.”
Adverse events associated with hepatitis B vaccine in U.S. children less than six years of age, 1993 and 1994. Fisher, et al. 2001
Controlling for age, race, and gender simultaneously in the 1994 NHIS, hepatitis B vaccine was found to be associated with prevalent arthritis [odds ratio (OR) = 5.91, 95% confidence interval (CI) = 1.05-33.14], incident acute ear infections (OR = 1.60, 95% CI = 1.00-2.58), and incident pharyngitis/nasopharyngitis (OR = 1.41, 95% CI = 0.95-2.09).
Recombinant hepatitis B vaccine and the risk of multiple sclerosis: A Prospective Study. Miguel A. Hernán, et al. 2004
Conclusions: These findings are consistent with the hypothesis that immunization with the recombinant hepatitis B vaccine is associated with an increased risk of MS, and challenge the idea that the relation between hepatitis B vaccination and risk of MS is well understood.
Hepatitis B vaccine associated with an increased risk of type 1 diabetes in Italy. P Pozzilli, et al. 2000
The development of rheumatoid arthritis after recombinant hepatitis B vaccination. Pope JE, et al 1998
Recombinant hepatitis B vaccine may trigger the development of RA in MHC class II genetically susceptible individuals.
2016
Haemophilus influenzae type b meningitis in a vaccinated and immunocompetent child Ana F Almeida et al. 2016
“We report a case of a fifteen-months-old girl, previously healthy and vaccinated, admitted in the emergency room with fever and vomiting. She was irritable and the Brudzinski’s sign was positive. Despite vaccination compliance and absence of risk factors, invasive Hib disease can occur due to vaccine failure.”
2013
Haemophilus influenzae type f meningitis in a previously healthy boy Andreas Ronit 2013
“We report a case of acute bacterial meningitis in a 14-year-old boy, who was previously healthy and had been immunised againstH influenzaeserotype b (Hib). The causative pathogen was identified asH influenzaeserotype f (Hif), and was successfully treated with ceftriaxone.”
2012
Haemophilus influenzae Type b Meningitis in the Short Period after Vaccination: A Reminder of the Phenomenon of Apparent Vaccine Failure Noa Greenberg-Kushnir 2012
We present two cases of bacterial meningitis caused by Haemophilus influenzae type b (Hib) which developed a few days after conjugate Hib vaccination. This phenomenon of postimmunization provocative time period is reviewed and discussed. These cases serve as a reminder to clinicians of the risk, albeit rare, of invasive Hib disease in the short period after successful immunization.
Case 1: A 10-week-old girl presented to another hospital with fever, refusal to eat, grunting respirations, and hypertonicity of 48-hour duration. All symptoms began one day after she had received the first dose of the combination Infanrix-IPV+Hib vaccine (a combined vaccine against diphtheria, tetanus, pertussis, polio, and Hib infections). Her parents reported that she had been perfectly healthy the day before vaccination.
Case 2: A 5-month-old boy presented to our hospital with fever, apathy, vomiting, and diarrhea of 24-hour duration. All symptoms began 6 days after he received the second dose of the Infanrix-IPV+Hib vaccine. His parents reported that he had been perfectly healthy on the day before vaccination.
Haemophilus influenzae and the lung (Haemophilus and the lung) Paul King. 2012
“H. influenzae is a component of the normal upper respiratory tract flora and is well recognized to be an important cause of systemic infection. It is also a major cause of a variety of respiratory conditions and has had a relatively low profile in this respect in comparison to some other pathogens; such as Mycobacterium tuberculosisand Streptococcuspneumoniae.”
“Recently there has been increasing recognition that this bacterium has a role in chronic lower respiratory tract inflammation. However the interaction between H. influenzae and the lung is still not well defined. A combination of bacterial pathogenic features and deficiency of host defense may permit this bacterium to establish infection in the lower respiratory tract resulting in inflammation and clinical disease. This review will discuss the role of H. influenzae in the lower respiratory tract in particular its role in bronchitis.”
2009
Breastfeeding protects against infectious diseases during infancy in industrialized countries. A systematic review Liesbeth Duijts 2009
“Four out of five studies observed decreased effects on overall infections in breastfed infants. With regard to gastrointestinal infections, six out of eight studies suggested that breastfeeding had a protective effect. Thirteen out of 16 studies concluded that breastfeeding protects infants against respiratory tract infections. Five studies combined duration and exclusiveness of breastfeeding. All studies observed a protective dose/duration-response effect on gastrointestinal or respiratory tract infections. These studies strongly suggest that breastfeeding protects infants against overall infections, gastrointestinal and respiratory tract infections in industrialized countries.”
2004
Incidence of Haemophilus influenzae type b and other invasive diseases in South Korean children. J S Kim 2004
“From September 1999 to December 2001, 2176 children were evaluated for possible meningitis, 1541 had no cerebrospinal fluid (CSF) findings of meningitis, 605 had CSF abnormalities (suspected bacterial meningitis) but no pathogen identified; six patients had probable Hib meningitis and eight had confirmed Hib meningitis. Hib vaccine coverage was negligible initially but increased to 16% (complete Hib immunization) and 27% (partial immunization) in final months of study. Suspected bacterial meningitis incidence was high but proven invasive Hib meningitis incidence was low. Hib was identified in only 4% of abnormal CSF.”
1999
Protective effect of breastfeeding: an ecologic study of Haemophilus influenzae meningitis and breastfeeding in a Swedish population S A Silfverdal 1999
“There seems to be an association between high breastfeeding rate in the population and a reduced incidence of HI meningitis 5 to 10 years later.”
1997
Protective effect of breastfeeding on invasive Haemophilus influenzae infection: a case-control study in Swedish preschool children S A Silfverdal 1997
“Multivariate analysis showed a significant association between invasive HI infection and two independent factors, i.e. short duration (< 13 weeks) of exclusive breastfeeding, odds ratio (OR) 3.79 (95% confidence interval [CI] 1.6-8.8) and history of frequent infections, OR 4.49 (95% CI : 1.0-21.0). For the age at onset 12 months or older, the associations were stronger, OR 7.79 (95% CI : 2.4-26.6) and 5.86 (95% CI : 1.1-30.6), respectively.”
Invasive Haemophilus influenzae Serotype f Case Reports in Mazovia Province, Poland
“Both patients were previously healthy, were not asplenic, they received all 4 doses of anti-Hib vaccination, and to our best knowledge, had no contact with anybody contagiously ill.”
2020
Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017-2018 influenza season. Greg G Wolff 2020
“Examining virus interference by specific respiratory viruses showed mixed results. Vaccine derived virus interference was significantly associated with coronavirus and human metapneumovirus.”
2018
Assessment of temporally-related acute respiratory illness following influenza vaccination. Rikin, et al. 2018
“Of the 999 participants, 68.8% were children, 30.2% were adults. Each study season, approximately half received influenza vaccine and one third experienced ≥1 ARI. The hazard of influenza in individuals during the 14-day post-vaccination period was similar to unvaccinated individuals during the same period (HR 0.96, 95% CI [0.60, 1.52]). The hazard of non-influenza respiratory pathogens was higher during the same period (HR 1.65, 95% CI [1.14, 2.38]); when stratified by age the hazard remained higher for children (HR 1·71, 95% CI [1.16, 2.53]) but not for adults (HR 0.88, 95% CI [0.21, 3.69]).
Among children there was an increase in the hazard of ARI caused by non-influenza respiratory pathogens post-influenza vaccination compared to unvaccinated children during the same period. Potential mechanisms for this association warrant further investigation.
Infectious virus in exhaled breath of symptomatic seasonal influenza cases from a college community. Jing Yan, et al. 2018
“Our observation of an association between repeated vaccination and increased viral aerosol generation demonstrated the power of our method, but needs confirmation.
2017
Influenza Vaccination in the First Trimester of Pregnancy and Risk of Autism Spectrum Disorder. Brian S Hooker 2017
Association of spontaneous abortion with receipt of inactivated influenza vaccine containing H1N1pdm09 in 2010-11 and 2011-12. Donahue JG, et al. 2017.
“SAB [spontaneous abortion] was associated with influenza vaccination in the preceding 28days. The association was significant only among women vaccinated in the previous influenza season with pH1N1-containing vaccine. This study does not and cannot establish a causal relationship between repeated influenza vaccination and SAB, but further research is warranted.
Association Between Influenza Infection and Vaccination During Pregnancy and Risk of Autism Spectrum Disorder. Ousseny Zerbo, PhD, et al. 2017
“In trimester-specific analyses, first-trimester influenza vaccination was the only period associated with increased ASD risk (adjusted hazard ratio, 1.20; 95% CI, 1.04-1.39). However, this association could be due to chance.
2015
Repeated flu shots may blunt effectiveness. Murray, Terry. 2015
2014
Impact of repeated vaccination on vaccine effectiveness against influenza A(H3N2) and B during 8 seasons. McLean et al. 2014
Current- and previous-season vaccination generated similar levels of protection, and vaccine-induced protection was greatest for individuals not vaccinated during the prior 5 years. Additional studies are needed to understand the long-term effects of annual vaccination.
Glossopharyngeal nerve and vagus nerve palsies associated with influenza vaccination. Ishii, et al. 2014
We herein report the first case of glossopharyngeal nerve and vagus nerve palsies that appeared after an influenza vaccination. A 15-year-old boy developed dysphagia and dysarthria seven days after receiving an inoculation of the inactivated influenza vaccine.
2012
Effectiveness of trivalent inactivated influenza vaccine in influenza-related hospitalization in children: a case-control study . Avni Y Joshi
“There was an overall trend toward higher rates of hospitalization in subjects who got the trivalent inactivated flu vaccine (TIV) when compared with the ones who did not get the TIV (odds ratio [OR], 3.67; CI, 1.6, 8.4) Using the Cochran-Mantel-Haenszel test for asthma status stratification, there was a significant association between hospitalization in asthmatic subjects and TIV (p = 0.001). TIV did not provide any protection against hospitalization in pediatric subjects, especially children with asthma. On the contrary, we found a threefold increased risk of hospitalization in subjects who did get the TIV vaccine. This may be a reflection not only of vaccine effectiveness but also the population of children who are more likely to get the vaccine.
“The daily incidence rate of an eventual seizure disorder diagnosis among those diagnosed with an initial seizure episode from 6 to 11 days post-MMR vaccination was significantly increased (unadjusted HR = 17.7, p < 0.01 and adjusted HR = 17.4, p < 0.01) in comparison to the daily incidence rate of an eventual seizure disorder diagnosis among those diagnosed with an initial seizure episode from 12 to 17 months among unvaccinated persons.
The current study revealed that about 1 in 3,100 doses of MMR vaccine administered to children from 12 through 16 months of age are attributably associated with a seizure disorder diagnosis following an initial seizure episode with an onset of symptoms from 6 to 11 days post-MMR vaccination.”
Adverse Events Following Measles, Mumps, and Rubella Vaccine in Adults Reported to the Vaccine Adverse Event Reporting System (VAERS), 2003–2013. Lakshmi Sukumaran, et al. 2015.
Results: During this period, VAERS received 3175 US reports after MMR vaccine in adults. Of these, 168 (5%) were classified as serious, including 7 reports of death. Females accounted for 77% of reports. The most common signs and symptoms for all reports were pyrexia (19%), rash (17%), pain (13%), and arthralgia (13%). We did not detect any new safety findings in empirical Bayesian data mining. We identified 131 reports of MMR vaccine administered to a pregnant woman; the majority of these vaccinations were in the first trimester and in 83 (62%), no AE was reported.
“Acetaminophen (paracetamol) use, measles-mumps-rubella vaccination, and autistic disorder: the results of a parent survey.” Schultz ST, et al. 2008
“Acetaminophen use after measles-mumps-rubella vaccination was significantly associated with autistic disorder when considering children 5 years of age or less (OR 6.11, 95% CI 1.42-26.3), after limiting cases to children with regression in development (OR 3.97, 95% CI 1.11-14.3), and when considering only children who had post-vaccination sequelae (OR 8.23, 95% CI 1.56-43.3), adjusting for age, gender, mother’s ethnicity, and the presence of illness concurrent with measles-mumps-rubella vaccination.”
MMR vaccine and idiopathic thrombocytopaenic purpura. Corri Black. 2003.
This study confirms the increased risk of ITP within 6 weeks after MMR vaccination. However, the attributable risk of ITP within 6 weeks after MMR vaccination is low.
“Elevated levels of measles antibodies in children with autism”. Singh VK, Jensen RL. 2003
“Abnormal measles-mumps-rubella antibodies and CNS autoimmunity in children with autism”. Singh VK, et al. 2002
Comparative Analysis of Titers of Antibody against Measles Virus in Sera of Vaccinated and Naturally Infected Japanese Individuals of Different Age Groups. Masae Itoh, et al. 2002.
This result suggests that the current vaccine strain would be suitable to elicit protection against types D3 and D5, as long as viral antigenicity is concerned. However, when compared at given hemagglutination inhibition titers, NT antibody titers of vaccinees were 21.1 to 23.2 times lower than those of naturally infected individuals, suggesting a qualitative difference(s) of anti-MV antibodies between the two groups. It should be emphasized that protective immunity induced by the one-dose vaccination currently implemented in Japan may not be strong enough to ensure lifelong immunity. A two-dose vaccination program with higher vaccination coverage needs to be considered in order to effectively control measles in Japan.
Detection and Sequencing of Measles Virus from Peripheral Mononuclear Cells from Patients with Inflammatory Bowel Disease and Autism. HISASHI KAWASHIMA, MD et al. 2000
Crohn’s Disease: Pathogenesis and Persistent Measles Virus Infection. ANDREW J. WAKEFIELD, et al. 1995
This section will have all studies related to MTHFR mutation (methylenetetrahydrofolate reductase mutation). This enzyme helps you convert one form of folate (5, 10-methylenetetrahydrofolate) to another form (5-methyltetrahydofolate, known as 5-MTHF). In the process of doing so, homocysteine is converted to methionine.
2020
Methylenetetrahydrofolate Reductase Deficiency: A Case Report. Hale, et al. 2020.
Methylenetetrahydrofolate reductase (MTHFR) deficiency is an autosomal recessive disorder that results in hyperhomocysteinemia. Elevated homocysteine levels in the blood can cause arterial and venous thrombosis, atherosclerosis, recurrent pregnancy loss, and neurologic symptoms. Emerging research suggests links to other chronic illnesses as well. Anesthetic management of patients with MTHFR deficiency should focus on decreasing the risk of arterial or venous thrombosis and minimizing elevations in homocysteine levels.
2017
Anesthetic management of a parturient with Methylene Tetrahydrofolate Reductase (MTHFR) mutations: A case report. Bisherwal, et al. 2017.
We present a case of pregnancy induced hypertension with MTHFR mutation successfully managed with regional anaesthesia.
2008
Genetic basis for adverse events after smallpox vaccination. Reif, et al. 2008. DOI: 10.1086/588670
The presence of a nonsynonymous SNP in the methylenetetrahydrofolate reductase (MTHFR)gene was associated with the risk ofAEin both trials (odds ratio [OR], 2.3 [95% confidence interval {CI}, 1.1-5.2] [P = .04] and OR, 4.1 [95% CI, 1.4 -11.4] [P<.01]).
2007
General anesthesia and methylenetetrahydrofolate reductase deficiency. Shay, et al. 2007.
Nitrous oxide use in anesthesia leads to significant increases in plasma homocysteine. We present a patient undergoing urgent surgery with a preoperative diagnosis of homozygous MTHFR deficiency.
2003
Nitrous Oxide Toxicity with Methylenetetrahydrofolate Reductase Deficiency. Millichap. 2003.
The neurological deterioration and death of a child with methylenetetrahydrofolate reductase (MTHFR) deficiency following anesthetization with nitrous oxide are reported from the University of Wisconsin Medical School, Madison, WI, and McGill University, Montreal.
The Introduction of Diphtheria-Tetanus-Pertussis and Oral Polio Vaccine Among Young Infants in an Urban African Community: A Natural Experiment. Mogensen, et al. 2017
Results: Among 3–5-month-old children, having received DTP (±OPV) was associated with a mortality hazard ratio (HR) of 5.00 (95% CI 1.53–16.3) compared with not-yet-DTP-vaccinated children. Differences in background factors did not explain the effect. The negative effect was particularly strong for children who had received DTPonly and no OPV (HR = 10.0 (2.61–38.6)). All-cause infant mortality after 3 months of age increased after the introduction of these vaccines (HR = 2.12 (1.07–4.19)).
Transmission of Imported Vaccine-Derived Poliovirus in an Undervaccinated Community in Minnesota. James P. Alexander, et al. 2008
Oral poliovirus vaccine (OPV) has not been used in the United States since 2000. Type 1 vaccine derived poliovirus (VDPV) was identified in September 2005, from an unvaccinated Amish infant hospitalized in Minnesota with severe combined immunodeficiency. An investigation was conducted to determine the source of the virus and its means of transmission.
Some oral poliovirus vaccines were contaminated with infectious SV40 after 1961. Cutrone, R., et al. 2005
These SV40-contaminated vaccines were produced from early 1960s to about 1978 and were used throughout the world. Our findings underscore the potential risks of using primary monkey cells for preparing poliovirus vaccines, because of the possible contamination with SV40 or other monkey viruses, and emphasize the importance of using well-characterized cell substrates that are free from adventitious agents.
A case of vaccine-associated paralytic poliomyelitis. Edwards, et al. 2000
We describe an episode of VAPP in an infant in whom paralysis became evident at age 124 days, 14 days after administration of the second dose of OPV vaccine. The second dose of diphtheria-tetanus-pertussis- Haemophilus (DTPH) type-b vaccine had been given at the time of OPV administration, and the hepatitis B vaccine had been administered in the opposite leg. Paralysis was localized to the limb in which the DTPH had been injected.
Cancer risk associated with simian virus 40 contaminated polio vaccine. Fisher, et al. 1999
The presence of SV40 in monkey cell cultures used in the preparation of the polio vaccine from 1955 through 1961 is well documented. Investigations have consistently demonstrated the oncogenic behavior of SV40 in animal models. Early epidemiologic studies were inadequate in demonstrating an increase in cancer incidence associated with contaminated vaccine. Recently, investigators have provided persuasive evidence that SV40 is present in human ependymomas, choroid plexus tumors, bone tumors, and mesotheliomas, however, the etiologic role of the virus in tumorigenesis has not been established.
Conclusions: These data suggest that there may be an increased incidence of certain cancers among the 98 million persons exposed to contaminated polio vaccine in the U.S.; further investigations are clearly justified.
Intramuscular Injections within 30 Days of Immunization with Oral Poliovirus Vaccine — A Risk Factor for Vaccine-Associated Paralytic Poliomyelitis, Peter M. Strebel, et al. 1995
Provocation paralysis, previously described only for wild-type poliovirus infection, may rarely occur in a child who receives multiple intramuscular injections shortly after exposure to oral poliovirus vaccine, either as a vaccine recipient or through contact with a recent recipient. This phenomenon may explain the high rate of vaccine-associated paralytic poliomyelitis in Romania, where the use of intramuscular injections of antibiotics in infants with febrile illness is common.
The findings of these early workers have been confirmed, and in addition it has been shown that alum-containing toxoid plus pertussis vaccine is outstandingly the most dangerous preparation, followed by precipitated toxoids and plain pertussis vaccine, all of which had approximately equal paralysis-provoking effect. Plain or fluid toxoid and TAF were the least provoking.
Poliomyelitis Following Inoculations, British Medical Journal. 1950
Systemic inflammatory reaction after pneumococcal vaccine. Kelley A von Elten, et al. 2014
Fever, leukocytosis, and large local reactions following the pneumococcal polysaccharide vaccine (PS23) have been described only in isolated case reports in the adult literature.
Protracted fever with cellulitis-like reaction in pneumococcal polysaccharide-vaccinated children. Daniel Tsung-Ning Huang 2008.
Side effects of the 23-valent pneumococcal polysaccharide vaccine (PPV23) are regarded as mild and uncommon in adults. In our clinical experience, however, protracted fever with a cellulitis-like reaction after PPV23 vaccination is not rare in pediatric patients. We reviewed the records of 17 children with those clinical findings after PPV23 vaccination.
Rotavirus shedding following administration of RV3-BB human neonatal rotavirus vaccine. Cowley, et al. 2017
Shedding of rotavirus was highest following vaccination at 8 weeks of age in both neonatal and infant schedules (19/30 and 17/27, respectively). Rotavirus was detected in stool on days 3–7, after at least one dose of RV3-BB, in 70% (21/30) of neonate, 78% (21/27) of infant and 3% (1/32) placebo participants.
Risk of Intussusception After Rotavirus Vaccination A Systematic Literature Review and Meta-Analysis. Judith Koch, Dr. 2017
RV vaccination is associated with a markedly elevated RR and a mildly elevated AR for intussusception 1–7 days after the first dose. Physicians should begin the series of vaccinations at age 6–12 weeks, as recommended by the STIKO, because the risk of intussusception is higher afterward. Current health insurance company claim data indicate that 11.2% of infants are still receiving the first dose of the vaccine at ages above 3 months. The parents of vaccinated children should be informed about the possible signs of intussusception (colicky pain, bilious vomiting, and red “currant jelly” stool).
Comparison of virus shedding after lived attenuated and pentavalent reassortant rotavirus vaccine. Yu-Chia Hsieh, et al. 2014
After the first vaccine dose, the peak time of virus shedding occurred between day 4 and day 7, with positive detection rates of 80-90% by real-time RT-PCR and 20-30% by EIA. In both groups, vaccine shedding occurred as early as one day and as late as 25-28 days.
An analysis of rotavirus vaccine reports to the vaccine adverse event reporting system: more than intussusception alone? Penina Haber, et al. 2004
Even after excluding intussusception cases, a higher proportion of RRV-TV reports than non-RRV-TV reports included fever and various gastrointestinal symptoms, most notably bloody stool but also vomiting, diarrhea, abdominal pain, gastroenteritis, abnormal stool, and dehydration.
Intussusception and gastroenteritis were the most commonly reported outcomes; however, a substantial number of reports indicate signs and symptoms consistent with either illness, possibly suggestive of a spectrum of gastrointestinal illness(es) related to RRV-TV.
Zoster vaccine-associated primary varicella infection in an immunocompetent host. Kaoru Harada, et al. 2017
A 64-year-old immunocompetent man developed a widespread pruritic and vesicular rash 2 weeks after receiving the zoster vaccine (Zostavax). He had fever, bandaemia with normal total white blood cell count and mild transaminitis. PCR testing of serum and skin was positive for varicella zoster virus (VZV), while serum VZV IgG was negative.
Varicella Zoster Virus DNA at Inoculation Sites and in Saliva After Zostavax Immunization. Duane L Pierson 2011
Analysis of 36 individuals over age 60 years who were immunized with Zostavax revealed varicella zoster virus (VZV) DNA in swabs of skin inoculation sites obtained immediately after immunization in 18 (50%) of 36 subjects (copy number per nanogram of total DNA, 28 to 2.1 × 106) and in saliva collected over 28 days in 21 (58%) of 36 subjects (copy number, 20 to 248). Genotypic analysis of DNA extracted from 9 random saliva samples identified vaccine virus in all instances. In some immunized individuals over age 60, vaccine virus DNA is shed in saliva up to 4 weeks.
Novel chemical-physical autopsy investigation in sudden infant death and sudden intrauterine unexplained death syndromes. Gatti, et al. 2022
Results: Developmental abnormalities of the brain were associated with the presence of foreign bodies. Although nanoparticles were present as well in control samples, they were not associated with histological brain anomalies, as was the case in SIDS/SIUDS.
Conclusion: Inorganic particles present in brain tissues demonstrate their ability to cross the hemato–encephalic barrier and to interact with tissues and cells in an unknown yet pathological fashion. This gives a rationale to consider them as cofactors of lethality.
“Some of the particles identified showed surprising amounts of aluminum alloys or aluminum and phosphorous…..The authors speculate that its sources could be aluminum cutlery, aluminum-containing pharmacy products or immunotherapy vaccines containing aluminum derivatives dissolved in Na–Cl, whose crystals are seen enriched with aluminum. Since the mother can transfer blood contaminants to her fetus, aluminum particles, known to be able to travel long distances, could have reached the brain tissues, as aluminum has a keen ‘tropism’ toward complex fatty tissues.”
Vaccines and sudden infant death: An analysis of the VAERS database 1990–2019 and review of the medical literature. Neil Z. Miller 2021
“Of 2605 infant deaths reported to VAERS from 1990 through 2019, 58 % clustered within 3 days post-vaccination and 78.3 % occurred within 7 days post-vaccination, confirming that infant deaths tend to occur in temporal proximity to vaccine administration. The excess of deaths during these early post-vaccination periods was statistically significant (p < 0.00001).”
Sudden Infant Death After Vaccination: Survey of Forensic Autopsy Files. Osawa, Motoki MD, PhD et al. 2019
Sudden infant deaths might be attributable to adverse reaction to vaccination, but separating them from coincidental occurrences is difficult…Of the 32 cases in which any vaccines were administered, 7 infants (21.9%) had received immunization within 7 days of death….Judgment of the disorders as truly related to vaccination is difficult, but suspicious cases do exist. Forensic pathologists must devote more attention to vaccination in sudden infant death cases.
Simultaneous sudden infant death syndrome: case report. Y Cevik, et al. 2017. Full text available here:twins dying of SIDS
Both babies had been vaccinated the second doses of oral polio vaccine, diphtheria-pertussis-tetanus and hepatitis B three days before death. The first baby had high fever and was given a full teaspoon (~40 mg) of ibuprofen syrup by the mother. Later, the fever settled according to the mother’s description.
“Infanrix hexa and sudden death: a review of the periodic safety update reports submitted to the European Medicines Agency” Jacob Puliyel, C Sathyamala. 2017
“The number of observed deaths soon after vaccination among children older than one year was significantly higher than that expected by chance once the deleted deaths were restored and included in the analysis.”
Sudden Infant Death With Area Postrema Lesion Likely Due to Wrong Use of Insecticide. Anna M. Lavezzi, et al. 2015
We report a noteworthy case of a 7-month-old infant who suddenly and unexpectedly died during her sleep. After a complete postmortem examination, review of the clinical history, and detailed death scene investigation, the death remained unexplained, leading to a diagnosis of sudden infant death syndrome. However, an extensive review of the brainstem neuropathology revealed a severe alteration in the area postrema (a highly vascular structure lying at the base of the fourth ventricle outside of the blood-brain barrier). The alteration was likely due to massive and repeated to a common household insecticide in the last few weeks of life. These results provide an explanation for this sudden infant death, allowing a differential diagnosis from sudden infant death syndrome.
Gut microbiota and immunity: possible role in sudden infant death syndrome. Paul N. Goldwater. 2015.
The aims of the review are to explore (1) the role of the gut microbiome in relation to the developmentally critical period in which most SIDS cases occur; (2) the mechanisms by which the gut microbiome might induce inflammation resulting in transit of bacteria from the lumen into the bloodstream; and (3) assessment of the clinical, physiological, pathological, and microbiological evidence for bacteremia leading to the final events in SIDS pathogenesis.
“DPT immunization and SIDS”. Kalyani Srinivas, G. Preeti, Sujatha Pasula. 2015
“It is found that mortality with SIDS in the period zero to three days following DTP to be 6.9 times that in the period beginning 30 days after immunization (95 per cent confidence interval, 1.4 to 28)”
“Pesticide exposure during pregnancy, like nicotine, affects the brainstem α7 nicotinic acetylcholine receptor expression, increasing the risk of sudden unexplained perinatal death”. Anna Maria Lavezzi, et al. 2014
We detain that exposition to pesticides in pregnancy produces homologous actions to those of nicotine on neuronal α7-nicotinic acetylcholine receptor, allowing to developmental alterations of brainstem vital centers in victims of sudden unexplained death.
“Sudden twin infant death on the same day: a case report and review of the literature” Huang, et. al. 2013 e.Huang et Twins
[Editors note: Ten week old twin infants received the first doses of oral polio and diphtheria, pertussis, and tetanus (DPT) vaccines 60 days after birth. So day 60 they were vaccinated and they died at 10 weeks, or day 70. Ten days after vaccination, twins died simultaneously on the same night.]
Sudden Infant Death Following Hexavalent Vaccination: A Neuropathologic Study. Matturri, et al. 2013 .Full Text of Hexavalent Vaccination Study
This study does not prove a causal relationship between the hexavalent vaccination and SIDS. However, we hypothesize that vaccine components could have a direct role in sparking off a lethal outcome in vulnerable babies. In conclusion, we sustain the need that deaths occurring in a short space of time after hexavalent vaccination are appropriately investigated and submitted to a post-mortem examination particularly of the autonomic nervous system by an expert pathologist to objectively evaluate the possible causative role of the vaccine in SIDS.
The association between multidose vaccinations and death: comparing case series methods when the first exposure changes the general risk of an event. Kuhnert, et al 2013
When we considered only vaccinated cases, the estimate increased to 2.21 (p value 0.001). We also observed a significantly higher risk of 1.51 (p value 0.044) for the general vaccination effect. Cox models estimated a significantly higher risk of 1.72 (p value 0.045) only for the first dose.
The Initial Common Pathway of Inflammation, Disease, and Sudden Death. Robert M. Davidson and Stephanie Seneff 2012.
Based on extensive review of the scientific literature, we propose in this paper that any exogenous substance that lowers the ZP, and/or introduces polycationic kosmotropic interfacial water stress, and/or lowers the bio-sulfate level, increases the likelihood of sudden death, by triggering a cascade of events in the pathogenesis of inflammation, allergy, infection, thrombosis, hemorrhage, ischemia, infarction, anaphylaxis, disease, and death. Inflammation, allergy, anaphylaxis, and serum sickness should be redefined to reflect this reality. A novel hypothesis as to the etiology of sudden death syndrome is presented which looks specifically at the very earliest events in the pathophysiology of SDS. In most instances, introduction of polycationic surfactants into our bloodstream causes acute interfacial water stress, lowering of ZP, lowering of pH, elevation of viscosity, and electrohemorheologic—hemodynamic derangement. This triggers a cascade of immunologic and hemostatic events, leading inexorably to tissue hypoperfusion, cellular anoxia, seizures, arrhythmias, infarctions, cardiovascular collapse, and death.
“Re-analyses of case-control studies examining the temporal association between sudden infant death syndrome and vaccination”. Ronny Kuhnert, et al. 2012 PDF here Reanalysis of case-control studies examining
“There is no increased or reduced risk of sudden infant death during the period after the vaccination. The previously reported protective effect seen in case control studies is based on the inclusion of unvaccinated cases.”
[Editor’s Note: This study erases any protective effect of vaccines regarding SIDS, because it only came to that conclusion by including a large majority of unvaccinated SIDS cases who died before reaching 2 months old, and thus died before they were eligible for vaccines. A vaccine cannot prevent a death that occurs before a vaccine would be routinely given. However, of infants who lived past 2 months old, they were 4 times more likely to be vaccinated prior to their death. Further research is needed to full understand the mechanism of SIDS, misdiagnosis, and the contributions of vaccines. Explore SIDS here.]
Sudden Unexpected Deaths and Vaccinations during the First Two Years of Life in Italy: A Case Series Study. Giuseppe Traversa, Stefania Spila-Alegiani, et. al. 2011.
Among the 604 infants who died of SUD, 244 (40%) had received at least one vaccination. Four deaths occurred within two days from vaccination with the hexavalent vaccines (RR = 1.5; 95% CI 0.6 to 4.2). The RRs for the risk periods 0–7 and 0–14 were 2.0 (95% CI 1.2 to 3.5) and 1.5 (95% CI 0.9 to 2.4). The increased risk was limited to the first dose (RR = 2.2; 95% CI 1.1 to 4.4), whereas no increase was observed for the second and third doses combined.
Sudden infant death syndrome: a case report in Bosnia and Herzegovina, Dragan Ćajić. 2010
A previously healthy 3 months old, white male infant was found dead after being placed to sleep in the prone position. The features of this case report closely parallel the classical features of SIDS cited in the world literature.
[Editors note: He was vaccinated 5 days before death.]
Cholinergic and oxidative stress mechanisms in sudden infant death syndrome. Anne Dick. 2009
Lower AChE levels and higher combined levels of iron and vitamin C in the first 6 months of life may augment cholinergic and oxidative stress effect, particularly at the age when SIDS is most prevalent. This may contribute to risk of ALTE and SIDS/SUDI events during infancy.
β-Tryptase and quantitative mast-cell increase in a sudden infant death following hexavalent immunization. StefanoD’Errico MargheritaNeri, et al. 2008.
“A fatal case of a 3-month-old female infant, who died within 24 h of vaccination with hexavalent vaccine is presented. Clinical data, post-mortem findings (acute pulmonary oedema, acute pulmonary emphysema), quali-quantitative data collected from immunohistochemical staining (degranulating mast cells) and laboratory analysis with a high level of β-tryptase in serum, 43.3 μg/l, allows us to conclude that acute respiratory failure likely due to post hexavalent immunization-related shock was the cause of death.”
Simultaneous sudden infant death syndrome. Balci Y., et al. 2007
The case(s): Twin girls (3.5-month-old) were found dead by their mother in their crib, both in supine position. The infants were identical twins and delivered at a hospital by cesarean section. Both infants were healthy and did not have any serious medical history. Two days prior to the incident, the twins had received the second dose of oral polio, DPT and the first dose of hepatitis B vaccines and they had fever on the first day of the vaccination and been given teaspoonful of acetaminophen. Death scene investigation, judicial investigation, parental assessment, macroscopic and microscopic autopsy findings and the toxicological analysis did not yield any specific cause of death.
An investigation of infant deaths following initial hepatitis B vaccination based on the Vaccine Adverse Event Reporting System (VAERS), 1992-2002. Soldatenkova, et al. 2007
“In most of the reviewed cases, the history, the symptoms and or the pathologic findings did not support the classification of death as unexplained or SIDS. All cases of “SIDS” occurring shortly after vaccination should be reported to VAERS.
The risks of vaccinating premature, small or slightly ill infants should be weighed against the benefits of each vaccine, particularly in cases where the vaccine is not even needed.
The role of low serum ascorbate in SIDS should be further investigated particularly since the number of recommended pediatric vaccines is constantly increasing.”
Letter to the Editor- Unexplained cases of sudden infant death shortly after hexavalent vaccination. 2006 Zinka FULL TEXT
We report six cases of sudden infant death after hexavalent vaccination…abnormal neuropathologic findings were acute congestion, defective blood-brain barrier, slight infiltration of the leptomeninx by macrophages and lymphocytes, perivascular lymphocytic infiltration, diffuse infiltration of the pons, mesencephalon and cortex by T lymphocytes, microglia in the hippocampus and pons, and in one cases a necrosis in the cerebellum.
Sudden infant death syndrome (SIDS) shortly after hexavalent vaccination: another pathology in suspected SIDS? Giulia Ottaviani, 2006.
Herein we report the case of a 3-month-old female infant dying suddenly and unexpectedly shortly after being given a hexavalent vaccination. Examination of the brainstem on serial sections revealed bilateral hypoplasia of the arcuate nucleus. The cardiac conduction system presented persistent fetal dispersion and resorptive degeneration. This case offers a unique insight into the possible role of hexavalent vaccine in triggering a lethal outcome in a vulnerable baby. Any case of sudden unexpected death occurring perinatally and in infancy, especially soon after a vaccination, should always undergo a full necropsy study according to our guidelines.
Pulmonary immunopathology of sudden infant death syndrome. W.J.HowatBSc, et al. 2003
The results showed three times more eosinophils in the lungs of infants who died of SIDS (27 61 vs 7·91 [99% Cl 1 76-5 87] cells/mm2 for parenchyma) accompanied by increased T lymphocytes and B lymphocytes. These findings provide evidence for an abnormal T lymphocyte-mediated pulmonary inflammatory response in SIDS. Products of eosinophil degranulation can cause epithelial damage and pulmonary oedema, which could cause the respiratory obstruction and hypoxia associated with SIDS.
Simultaneous sudden infant death syndrome: a case report. Ladham S, et al. 2001
The first reported case of simultaneous sudden infant death syndrome (SSIDS) in Allegheny County, Pennsylvania, occurred on February 27, 1998. Two-month-old black fraternal twin girls were both found dead in their crib at the same time. After an in-depth death scene investigation, police investigation, toxicologic analysis, and complete autopsies, a specific cause of death could not be identified. The deaths of the two girls were therefore ruled simultaneous sudden infant death syndrome.
Sudden infant death syndrome and diphtheria‐tetanus‐pertussis‐poliomyelitis vaccination status. Jonville-Bera, et al. 1995
The vaccination status of 118 SIDS and 332 control children, matched for sex, date of birth and age of the victims at death, was compared: the victims of SIDS were not significantly more often vaccinated than control children, the odds ratio was estimated at 1.9 with a 95% confidence interval from 0.9 to 3.9. There was a statistical difference between vaccination status of SIDS cases and controls aged less than three months. Nine percent of SIDS cases under 3 months had been vaccinated whereas the matched controls had not. In our study DTCP vaccination was not a risk factor for SIDS; although more of the SIDS infants less than 3 months of age had been vaccinated.
Involvement of mast cells in sudden infant death syndrome. Platt, MD, et al. 1994
An infant with SIDS had a 20-fold higher chance of having an elevated tryptase level compared with a control infant. Recognition of this pathway as operative in SIDS should facilitate a more precise identification of the allergens involved, the processes leading to mast cell activation, and procedures to identify those infants at risk for anaphylaxis, and should, in time, lead to better therapeutic interventions aimed at preventing this specific cause of SIDS.
Evidence Concerning Pertussis Vaccines and Deaths Classified as Sudden Infant Death Syndrome. Institute of Medicine report 1991
Case reports of SIDS include the deaths of 5- and 10-month-old twins within 3 and 24 hours, respectively, of DPT immunization (Roberts, 1987; Werne and Garrow, 1946). Episodes of death following administration of DPT vaccine were reported for six additional children, five of whom died within 48 hours of immunization (Coulter and Fisher, 1985). Torch (1986) summarized case reports of more than 150 deaths, post-DPT immunization, which had been reported by 37 authors in 12 countries; approximately 50 percent of these deaths occurred within 24 hours, 75 percent within 72 hours, and 90 percent within 1 week following DPT administration. For most of these events, no specific cause of death could be found, and many of these cases were designated as SIDS. (This summary of case reports was published in abstract form only.)
“Diphtheria-Tetanus-Pertussis Immunization and Sudden Infant Death Syndrome”. Walker, et al. 1987
“Focusing on very narrow time intervals following immunization, we found the SIDS mortality rate in the period zero to three days following DTP to be 7.3 times that in the period beginning 30 days after immunization (95 per cent confidence interval, 1.7 to 31).”
Vaccination and cot deaths in perspective. Roberts 1987
In 1985 twin boys simultaneously succumbed to sudden unexpected deaths two to three hours after vaccination with diphtheria, tetanus, and pertussis vaccine (DTP). This occurrence again raises the question of whether an association of sudden infant death (SID) with vaccination is other than temporal.
Possible temporal association between diphtheria-tetanus toxoid-pertussis vaccination and sudden infant death syndrome. Baraff, et al. 1983
Fifty-three had received a DTP immunization. Of these 53, 27 had received a DTP immunization within 28 days of death. Six SIDS deaths occurred within 24 hours and 17 occurred within 1 week of DTP immunization. These SIDS deaths were significantly more than expected were there no association between DTP immunization and SIDS. An additional 46 infants had a physician/clinic visit without DTP immunization prior to death. Forty of these infants died within 28 days of this visit, seven on the third day and 22 within the first week following the visit. These deaths were also significantly more than expected. These data suggest a temporal association between DTP immunization, physician visits without DTP immunization and SIDS.
a- and B-Tryptase Levels in Near-Miss Sudden Infant Death Syndrome (SIDS) Patients. AD Hogan, MD.
Further evaluation of near-miss SIDS infants with abnormal levels of a and b-tryptase could help to discern which infants are at increased risk of sudden infant death syndrome, and what might cause mast cell activation.
2017
Temporal Association of Certain Neuropsychiatric Disorders Following Vaccination of Children and Adolescents: A Pilot Case-Control Study. Leslie, et al. 2017
Subjects with newly diagnosed AN were more likely than controls to have had any vaccination in the previous 3 months [hazard ratio (HR) 1.80, 95% confidence interval 1.21-2.68]. Influenza vaccinations during the prior 3, 6, and 12 months were also associated with incident diagnoses of AN (anorexia nervosa), OCD (obsessive-compulsive disorder), and an anxiety disorder. Several other associations were also significant with HRs greater than 1.40 (hepatitis A with OCD and AN; hepatitis B with AN; and meningitis with AN and chronic tic disorder).
Abating Mercury Exposure in Young Children Should Include Thimerosal-Free Vaccines. Jose Dorea, 2017
Thimerosal-free vaccines have shown a decrease in contact dermatitis, while TCVs showed a significant association with increased risk of tic disorders; in some circumstances, EtHg in combination with other neurotoxic substances negatively impacted neurobehavioral tests. In studies that explored vaccines and risk of tics, Thimerosal was a necessary factor.
2015
Thimerosal exposure and increased risk for diagnosed tic disorder in the United States: a case-control study. Geier, et a. 2015
Although routine childhood vaccination is considered an important public health tool to combat infectious diseases, the present study associates increasing organic-Hg exposure from TM-HepB and the subsequent risk of a TD diagnosis.
2014
The role of immune mechanisms in Tourette syndrome. Martino, et al. 2014
An involvement of immune mechanisms in its pathophysiology has been proposed. Animal models based on active immunization with bacterial or viral mimics, direct injection of cytokines or patients’ serum anti-neuronal antibodies, and transgenic approaches replicated stereotyped behaviors observed in human TS.
Letter from Siri Glimstad “Re: Vaccinated vs. unvaccinated health outcomes in Ulster children” Letter to NY DOH_2021_05_21
Verified Court Petition from The Control Group Litigation attorneys Greg Glaser and Ray Flores. tcg-first-amended-verified-petition
“Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination.”
“Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disorders.” Brian S. Hooker, Neil Z. Miller. 2020.
“Pilot comparative study on the health of vaccinated and unvaccinated 6- to 12-year-old U.S. children.” Anthony R Mawson 2017.
“Childhood vaccine status and correlation with common nonvaccine-preventable illnesses.” Michelle M. Anderson DNP, FNP. 2017.
“Increased Risk of Noninfluenza Respiratory Virus Infections Associated With Receipt of Inactivated Influenza Vaccine.” Benjamin J. Cowling. 2012.
Vaccinated VS. Unvaccinated Studies
Letter from Siri Glimstad “Re: Vaccinated vs. unvaccinated health outcomes in Ulster children” Letter to NY DOH_2021_05_21
Verified Court Petition from The Control Group Litigation attorneys Greg Glaser and Ray Flores. tcg-first-amended-verified-petition
“Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination.”
“Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disorders.” Brian S. Hooker, Neil Z. Miller. 2020.
“Pilot comparative study on the health of vaccinated and unvaccinated 6- to 12-year-old U.S. children.” Anthony R Mawson 2017.
“Childhood vaccine status and correlation with common nonvaccine-preventable illnesses.” Michelle M. Anderson DNP, FNP. 2017.
“Increased Risk of Noninfluenza Respiratory Virus Infections Associated With Receipt of Inactivated Influenza Vaccine.” Benjamin J. Cowling. 2012.
Aluminium in brain tissue in autism. Matthew Mold, Dorcas Umar, Andrew King, Christopher Exley. 2018
While aluminium was imaged associated with neurones it appeared to be present intracellularly in microglia-like cells and other inflammatory non-neuronal cells in the meninges, vasculature, grey and white matter. The pre-eminence of intracellular aluminium associated with nonneuronal cells was a standout observation in autism brain tissue and may offer clues as to both the origin of the brain aluminium as well as a putative role in autism spectrum disorder.
“Immunoexcitotoxicity as the central mechanism of etiopathology and treatment of autism spectrum disorders: A possible role of fluoride and aluminum” Anna Strunecka, Russell L. Blaylock, Jiri Patocka, and Otakar Strunecky. 2018
“We demonstrate that fluoride and aluminum (Al3+) can exacerbate the pathological problems by worsening excitotoxicity and inflammation. While Al3+ appears among the key suspicious factors of ASD, fluoride is rarely recognized as a causative culprit. A long-term burden of these ubiquitous toxins has several health effects with a striking resemblance to the symptoms of ASD.”
Association Between Influenza Infection and Vaccination During Pregnancy and Risk of Autism Spectrum Disorder. Ousseny Zerbo, PhD, et al. 2017
In trimester-specific analyses, first-trimester influenza vaccination was the only period associated with increased ASD risk (adjusted hazard ratio, 1.20; 95% CI, 1.04-1.39). However, this association could be due to chance.
Maternal breastfeeding and autism spectrum disorder in children: A systematic review and meta-analysis. Tseng PT 2017
This meta-analysis provides evidence that breastfeeding (exclusively or including additional supplements) may protect against ASD. Prospective longitudinal research is required to disentangle the complex relationships and to explore potential pathophysiological mechanisms.
“Vaccines are not associated with autism: An evidence-based meta-analysis of case-control and cohort studies” Luke E. Taylor, Amy L. Swerdfeger, Guy D. Eslick. 2014
“Studies were included that looked at either MMR vaccination, cumulative mercury (Hg) or cumulative thimerosal dosage from vaccinations to ensure all proposed causes of ASD or regression were investigated.”
[Editor’s note: Please take special note that only MMR vaccine, and or cumulative mercury exposure, was investigated before coming to the conclusion that ALL VACCINES are not associated with Autism. Please see further articles here.]
“Transcriptomic analyses of neurotoxic effects in mouse brain after intermittent neonatal administration of thimerosal.” Li X,Qu F,Xie W, et al. 2014
“Thimerosal-treated mice exhibited neural development delay, social interaction deficiency, and inclination of depression.”
“Methodological Issues and Evidence of Malfeasance in Research Purporting to Show Thimerosal in Vaccines Is Safe”. Brian Hooker, et al. 2014
Assessment of Infantile Mineral Imbalances in Autism Spectrum Disorders (ASDs). Hiroshi Yasuda and Toyoharu Tsutsui. 2013.
These findings suggest that infantile zinc- and magnesium-deficiency and/or toxic metal burdens may be critical and induce epigenetic alterations in the genes and genetic regulation mechanisms of neurodevelopment in the autistic children, and demonstrate that a time factor “infantile window” is also critical for neurodevelopment and probably for therapy.
“Maternal immune activation causes age and region-specific changes in brain cytokines in offspring throughout development.” Garay, Paula A. Hsiao, Elaine Y. Patterson, Paul H. McAllister, A K. Brain, behavior, and immunity 2013; 31():54-68 PubMed Link
“Together, these data indicate that MIA leads to long-lasting, region-specific changes in brain cytokines in offspring—similar to those reported for ASD and SZ—that may alter CNS development and behavior.”
Toxic Metals and Essential Elements in Hair and Severity of Symptoms among Children with Autism. Eleonor BLAUROCK-BUSCH. 2012
Our data supports the historic evidence that heavy metals play a role in the development of ASD. In combination with an inadequate nutritional status the toxic effect of metals increase along with the severity of symptoms.
“Hypothesis: conjugate vaccines may predispose children to autism spectrum disorders.“ Richmand BJ. Med Hypotheses. 2011.
Conjugate vaccines fundamentally change the manner in which the immune systems of infants and young children function by deviating their immune responses to the targeted carbohydrate antigens from a state of hypo-responsiveness to a robust B2 B cell mediated response. This period of hypo-responsiveness to carbohydrate antigens coincides with the intense myelination process in infants and young children, and conjugate vaccines may have disrupted evolutionary forces that favored early brain development over the need to protect infants and young children from capsular bacteria.
“A positive association found between autism prevalence and childhood vaccination uptake across the U.S. population”. Delong G. 2011
“A positive and statistically significant relationship was found: The higher the proportion of children receiving recommended vaccinations, the higher was the prevalence of AUT or SLI. A 1% increase in vaccination was associated with an additional 680 children having AUT or SLI.”
“Hepatitis B vaccination of male neonates and autism diagnosis, NHIS 1997-2002″. Gallagher CM, Goodman MS. 2010
“Findings suggest that U.S. male neonates vaccinated with the hepatitis B vaccine prior to 1999 (from vaccination record) had a threefold higher risk for parental report of autism diagnosis compared to boys not vaccinated as neonates during that same time period.”
“Immune-glutamatergic dysfunction as a central mechanism of the autism spectrum disorders”. Blaylock RL, Strunecka A. 2009
“We suggest that environmental and dietary excitotoxins, mercury, fluoride, and aluminum can exacerbate the pathological and clinical problems by worsening excitotoxicity and by microglial priming.”
“What is regressive autism and why does it occur? Is it the consequence of multi-systemic dysfunction affecting the elimination of heavy metals and the ability to regulate neural temperature?” Graham E. Ewing. 2009
This article explores the issues and concludes that sensory dysfunction and systemic failure, manifested as autism, is the inevitable consequence arising from subtle DNA alteration and consequently from the overuse of vaccines.
“Acetaminophen (paracetamol) use, measles-mumps-rubella vaccination, and autistic disorder: the results of a parent survey.” Schultz ST, et al. 2008
“Acetaminophen use after measles-mumps-rubella vaccination was significantly associated with autistic disorder when considering children 5 years of age or less (OR 6.11, 95% CI 1.42-26.3), after limiting cases to children with regression in development (OR 3.97, 95% CI 1.11-14.3), and when considering only children who had post-vaccination sequelae (OR 8.23, 95% CI 1.56-43.3), adjusting for age, gender, mother’s ethnicity, and the presence of illness concurrent with measles-mumps-rubella vaccination.”
“Maternal Immune Activation Alters Fetal Brain Development through Interleukin-6”. Stephen E. P. Smith, Jennifer Li, Krassimira Garbett, Karoly Mirnics, and Paul H. Patterson. 2007
A prospective study of thimerosal-containing Rho(D)-immune globulin administration as a risk factor for autistic disorders. Geier DA, Geier MR. 2007
“Children with ASDs (28.30%) were significantly more likely (odds ratio 2.35, 95% confidence interval 1.17-4.52, p < 0.01) to have Rh-negative mothers than controls (14.36%). Each ASD patient’s mother was determined to have been administered a TCR during her pregnancy.”
Environmental mercury release, special education rates, and autism disorder: an ecological study of Texas, Raymond F. Palmera, 2006
On average, for each 1000 lb of environmentally released mercury, there was a 43% increase in the rate of special education services and a 61% increase in the rate of autism. The association between environmentally released mercury and special education rates were fully mediated by increased autism rates. This ecological study suggests the need for further research regarding the association between environmentally released mercury and developmental disorders such as autism. These results have implications for policy planning and cost analysis.
Breastfeeding, infant formula supplementation, and Autistic Disorder: the results of a parent survey. Stephen T Schultz 2006
The results of this preliminary study indicate that children who were not breastfed or were fed infant formula without docosahexaenoic acid/arachidonic acid supplementation were significantly more likely to have autistic disorder.
“Immunological findings in autism”. Cohly HH, Panja A. 2005
“Elevated levels of measles antibodies in children with autism”. Singh VK, Jensen RL. 2003
“Abnormal measles-mumps-rubella antibodies and CNS autoimmunity in children with autism”. Singh VK, et al. 2002
The Introduction of Diphtheria-Tetanus-Pertussis and Oral Polio Vaccine Among Young Infants in an Urban African Community: A Natural Experiment. Mogensen, et al. 2017
Results: Among 3–5-month-old children, having received DTP (±OPV) was associated with a mortality hazard ratio (HR) of 5.00 (95% CI 1.53–16.3) compared with not-yet-DTP-vaccinated children. Differences in background factors did not explain the effect. The negative effect was particularly strong for children who had received DTPonly and no OPV (HR = 10.0 (2.61–38.6)). All-cause infant mortality after 3 months of age increased after the introduction of these vaccines (HR = 2.12 (1.07–4.19)).
Transmission of Imported Vaccine-Derived Poliovirus in an Undervaccinated Community in Minnesota. James P. Alexander, et al. 2008
Oral poliovirus vaccine (OPV) has not been used in the United States since 2000. Type 1 vaccine derived poliovirus (VDPV) was identified in September 2005, from an unvaccinated Amish infant hospitalized in Minnesota with severe combined immunodeficiency. An investigation was conducted to determine the source of the virus and its means of transmission.
Some oral poliovirus vaccines were contaminated with infectious SV40 after 1961. Cutrone, R., et al. 2005
These SV40-contaminated vaccines were produced from early 1960s to about 1978 and were used throughout the world. Our findings underscore the potential risks of using primary monkey cells for preparing poliovirus vaccines, because of the possible contamination with SV40 or other monkey viruses, and emphasize the importance of using well-characterized cell substrates that are free from adventitious agents.
Cancer risk associated with simian virus 40 contaminated polio vaccine. Fisher, et al. 1999
The presence of SV40 in monkey cell cultures used in the preparation of the polio vaccine from 1955 through 1961 is well documented. Investigations have consistently demonstrated the oncogenic behavior of SV40 in animal models. Early epidemiologic studies were inadequate in demonstrating an increase in cancer incidence associated with contaminated vaccine. Recently, investigators have provided persuasive evidence that SV40 is present in human ependymomas, choroid plexus tumors, bone tumors, and mesotheliomas, however, the etiologic role of the virus in tumorigenesis has not been established.
Conclusions: These data suggest that there may be an increased incidence of certain cancers among the 98 million persons exposed to contaminated polio vaccine in the U.S.; further investigations are clearly justified.
Intramuscular Injections within 30 Days of Immunization with Oral Poliovirus Vaccine — A Risk Factor for Vaccine-Associated Paralytic Poliomyelitis, Peter M. Strebel, et al. 1995
Provocation paralysis, previously described only for wild-type poliovirus infection, may rarely occur in a child who receives multiple intramuscular injections shortly after exposure to oral poliovirus vaccine, either as a vaccine recipient or through contact with a recent recipient. This phenomenon may explain the high rate of vaccine-associated paralytic poliomyelitis in Romania, where the use of intramuscular injections of antibiotics in infants with febrile illness is common.
“The daily incidence rate of an eventual seizure disorder diagnosis among those diagnosed with an initial seizure episode from 6 to 11 days post-MMR vaccination was significantly increased (unadjusted HR = 17.7, p < 0.01 and adjusted HR = 17.4, p < 0.01) in comparison to the daily incidence rate of an eventual seizure disorder diagnosis among those diagnosed with an initial seizure episode from 12 to 17 months among unvaccinated persons.
The current study revealed that about 1 in 3,100 doses of MMR vaccine administered to children from 12 through 16 months of age are attributably associated with a seizure disorder diagnosis following an initial seizure episode with an onset of symptoms from 6 to 11 days post-MMR vaccination.”
Adverse Events Following Measles, Mumps, and Rubella Vaccine in Adults Reported to the Vaccine Adverse Event Reporting System (VAERS), 2003–2013. Lakshmi Sukumaran, et al. 2015.
Results: During this period, VAERS received 3175 US reports after MMR vaccine in adults. Of these, 168 (5%) were classified as serious, including 7 reports of death. Females accounted for 77% of reports. The most common signs and symptoms for all reports were pyrexia (19%), rash (17%), pain (13%), and arthralgia (13%). We did not detect any new safety findings in empirical Bayesian data mining. We identified 131 reports of MMR vaccine administered to a pregnant woman; the majority of these vaccinations were in the first trimester and in 83 (62%), no AE was reported.
“Acetaminophen (paracetamol) use, measles-mumps-rubella vaccination, and autistic disorder: the results of a parent survey.” Schultz ST, et al. 2008
“Acetaminophen use after measles-mumps-rubella vaccination was significantly associated with autistic disorder when considering children 5 years of age or less (OR 6.11, 95% CI 1.42-26.3), after limiting cases to children with regression in development (OR 3.97, 95% CI 1.11-14.3), and when considering only children who had post-vaccination sequelae (OR 8.23, 95% CI 1.56-43.3), adjusting for age, gender, mother’s ethnicity, and the presence of illness concurrent with measles-mumps-rubella vaccination.”
MMR vaccine and idiopathic thrombocytopaenic purpura. Corri Black. 2003.
This study confirms the increased risk of ITP within 6 weeks after MMR vaccination. However, the attributable risk of ITP within 6 weeks after MMR vaccination is low.
“Elevated levels of measles antibodies in children with autism”. Singh VK, Jensen RL. 2003
“Abnormal measles-mumps-rubella antibodies and CNS autoimmunity in children with autism”. Singh VK, et al. 2002
Comparative Analysis of Titers of Antibody against Measles Virus in Sera of Vaccinated and Naturally Infected Japanese Individuals of Different Age Groups. Masae Itoh, et al. 2002.
This result suggests that the current vaccine strain would be suitable to elicit protection against types D3 and D5, as long as viral antigenicity is concerned. However, when compared at given hemagglutination inhibition titers, NT antibody titers of vaccinees were 21.1 to 23.2 times lower than those of naturally infected individuals, suggesting a qualitative difference(s) of anti-MV antibodies between the two groups. It should be emphasized that protective immunity induced by the one-dose vaccination currently implemented in Japan may not be strong enough to ensure lifelong immunity. A two-dose vaccination program with higher vaccination coverage needs to be considered in order to effectively control measles in Japan.
Detection and Sequencing of Measles Virus from Peripheral Mononuclear Cells from Patients with Inflammatory Bowel Disease and Autism. HISASHI KAWASHIMA, MD et al. 2000
Crohn’s Disease: Pathogenesis and Persistent Measles Virus Infection. ANDREW J. WAKEFIELD, et al. 1995
Evidence of Increase in Mortality After the Introduction of Diphtheria-Tetanus-Pertussis Vaccine to Children Aged 6-35 Months in Guinea-Bissau: A Time for Reflection? Aaby, Peter, et al. 2018
Although having better nutritional status and being protected against three infections, 6-35 months old DTP-vaccinated children tended to have higher mortality than DTP-unvaccinated children. All studies of the introduction of DTP have found increased overall mortality.
The Introduction of Diphtheria-Tetanus-Pertussis and Oral Polio Vaccine Among Young Infants in an Urban African Community: A Natural Experiment. Mogensen, et al. 2017
Results: Among 3–5-month-old children, having received DTP (±OPV) was associated with a mortality hazard ratio (HR) of 5.00 (95% CI 1.53–16.3) compared with not-yet-DTP-vaccinated children. Differences in background factors did not explain the effect. The negative effect was particularly strong for children who had received DTPonly and no OPV (HR = 10.0 (2.61–38.6)). All-cause infant mortality after 3 months of age increased after the introduction of these vaccines (HR = 2.12 (1.07–4.19)).
Asymptomatic transmission and the resurgence of Bordetella pertussis. Benjamin M. Althouse. 2015
Although a clear role for the previously suggested mechanisms still exists, asymptomatic transmission is the most parsimonious explanation for many of the observations surrounding the resurgence of B. pertussis in the US and UK.
Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model. Jason M. Warfel, et al. 2013
Baboons vaccinated with aP were protected from severe pertussis-associated symptoms but not from colonization, did not clear the infection faster than naïve animals, and readily transmitted B. pertussis to unvaccinated contacts.
Anti-NMDA receptor encephalitis after TdaP–IPV booster vaccination: cause or coincidence? Caroline Hofmann, et al. 2011.
We report about a 15-year-old female patient who was diagnosed with anti-NMDA receptor encephalitis after receiving a booster vaccination against tetanus/diphtheria/ pertussis and polio (TdaP-IPV).
Delay in diphtheria, pertussis, tetanus vaccination is associated with a reduced risk of childhood asthma. Kara L. McDonald, MSc, et al. 2008.
We found a negative association between delay in administration of the first dose of whole-cell DPT immunization in childhood and the development of asthma; the association was greater with delays in all of the first 3 doses. The mechanism for this phenomenon requires further research.
Deaths related to the injection of foreign protein in man are fortunately few. The exact number of such occurrences is difficult to estimate from the available literature. By 1942 Kojis1 was able to find 61 such deaths, and he added 4 more from the Willard Parker Hospital. The most complete and most recent study of necropsies was made by Vance and Strassmann,2 who added 7 autopsy studies from the Office of the Chief Medical Examiner to 19 taken from the literature. Park3 in 1932 recorded the mortality from serum anaphylaxis as 0.002 per cent. Kojis1 in 1942 found it to be just under 0.1 per cent in a series of 6,211 subjects treated for various infections. Rutstein and his associates,4 in their analysis of pneumonia cases treated with antipneumococcus horse serum, found the mortality to be 0.45 per cent. In only 1 or possibly 2
Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017-2018 influenza season. Greg G Wolff 2020
“Examining virus interference by specific respiratory viruses showed mixed results. Vaccine derived virus interference was significantly associated with coronavirus and human metapneumovirus.”
Assessment of temporally-related acute respiratory illness following influenza vaccination. Rikin, et al. 2018
Of the 999 participants, 68.8% were children, 30.2% were adults. Each study season, approximately half received influenza vaccine and one third experienced ≥1 ARI. The hazard of influenza in individuals during the 14-day post-vaccination period was similar to unvaccinated individuals during the same period (HR 0.96, 95% CI [0.60, 1.52]). The hazard of non-influenza respiratory pathogens was higher during the same period (HR 1.65, 95% CI [1.14, 2.38]); when stratified by age the hazard remained higher for children (HR 1·71, 95% CI [1.16, 2.53]) but not for adults (HR 0.88, 95% CI [0.21, 3.69]).
Among children there was an increase in the hazard of ARI caused by non-influenza respiratory pathogens post-influenza vaccination compared to unvaccinated children during the same period. Potential mechanisms for this association warrant further investigation.
Infectious virus in exhaled breath of symptomatic seasonal influenza cases from a college community. Jing Yan, et al. 2018
Our observation of an association between repeated vaccination and increased viral aerosol generation demonstrated the power of our method, but needs confirmation.
Association of spontaneous abortion with receipt of inactivated influenza vaccine containing H1N1pdm09 in 2010-11 and 2011-12. Donahue JG, et al. 2017.
SAB [spontaneous abortion] was associated with influenza vaccination in the preceding 28days. The association was significant only among women vaccinated in the previous influenza season with pH1N1-containing vaccine. This study does not and cannot establish a causal relationship between repeated influenza vaccination and SAB, but further research is warranted.
Association Between Influenza Infection and Vaccination During Pregnancy and Risk of Autism Spectrum Disorder. Ousseny Zerbo, PhD, et al. 2017
In trimester-specific analyses, first-trimester influenza vaccination was the only period associated with increased ASD risk (adjusted hazard ratio, 1.20; 95% CI, 1.04-1.39). However, this association could be due to chance.
Effectiveness of trivalent inactivated influenza vaccine in influenza-related hospitalization in children: a case-control study . Avni Y Joshi
There was an overall trend toward higher rates of hospitalization in subjects who got the trivalent inactivated flu vaccine (TIV) when compared with the ones who did not get the TIV (odds ratio [OR], 3.67; CI, 1.6, 8.4) Using the Cochran-Mantel-Haenszel test for asthma status stratification, there was a significant association between hospitalization in asthmatic subjects and TIV (p = 0.001). TIV did not provide any protection against hospitalization in pediatric subjects, especially children with asthma. On the contrary, we found a threefold increased risk of hospitalization in subjects who did get the TIV vaccine. This may be a reflection not only of vaccine effectiveness but also the population of children who are more likely to get the vaccine.
Severe Herpes Zoster Following Varicella Vaccination in Immunocompetent Young Children. Moodley A 2019.
Since varicella vaccine is a live attenuated virus, the virus replicates in the skin after administration and can travel via sensory nerves or viremia to become latent in the dorsal root ganglia. In some immunized children, virus reactivates within a few months to a few years to cause the dermatomal exanthem known as herpes zoster (shingles).
One of the children with herpes zoster subsequently developed asthma, a known risk factor for herpes zoster, but none of the children had an autoimmune disease. Although postherpetic neuralgia is exceedingly rare, children who develop herpes zoster following varicella vaccination are at risk (albeit low) of developing meningoencephalitis and should be carefully observed for a few weeks.
Neonatal varicella: Probable transmission from a vaccinated mother. Hajime Machi, et al. 2018.
History of chickenpox in glioma risk: a report from the glioma international case–control study (GICC). E. Susan Amirian, et al. 2016.
Here, we utilized the GICC data to confirm the previously reported associations between history of chickenpox and glioma risk in one of the largest studies to date on this topic. Using two-stage random-effects restricted maximum likelihood modeling, we found that a positive history of chickenpox was associated with a 21% lower glioma risk, adjusting for age and sex (95% confidence intervals (CI): 0.65–0.96). Furthermore, the protective effect of chickenpox was stronger for high-grade gliomas. Our study provides additional evidence that the observed protective effect of chickenpox against glioma is unlikely to be coincidental.
Transmission of varicella vaccine virus to a non-family member in China. Lin Gan, et al. 2011.
Transmission of varicella-vaccine virus from a healthy 12-month-old child to his pregnant mother. Salzman MB, et al. 1997
A 12-month-old healthy boy had approximately 30 vesicular skin lesions 24 days after receiving varicella vaccine. Sixteen days later his pregnant mother had 100 lesions. Varicella-vaccine virus was identified by polymerase chain reaction in the vesicular lesions of the mother. After an elective abortion, no virus was detected in the fetal tissue. This case documents transmission of varicella-vaccine virus from a healthy 12-month-old infant to his pregnant mother.
Inflammatory Arthritis following Hepatitis B Vaccination in an Infant. Sana S. Rahimi. 2021
“Herein, we describe the first reported case of an infant who developed inflammatory arthritis following hepatitis B vaccination. A 10-day-old female presented for evaluation of decreased movement of the right lower extremity and right knee swelling. Of note, the patient received a hepatitis B vaccine in her right thigh at birth. A workup found the patient to have a negative ANA but the presence of HLA B27.”
Premature Puberty and Thimerosal-Containing Hepatitis B Vaccination: A Case-Control Study in the Vaccine Safety Datalink. Geier, et al. 2018
The results of this study show a dose-dependent association between increasing organic Hg exposure from Thimerosal-containing hepatitis B vaccines administered within the first six months of life and the long-term risk of the child being diagnosed with premature puberty.
Hepatitis B vaccination of male neonates and autism diagnosis, NHIS 1997-2002. Gallagher, et al. 2010.
Findings suggest that U.S. male neonates vaccinated with thehepatitis B vaccineprior to 1999 (from vaccination record) had a threefold higher risk for parental report of autism diagnosis compared to boys not vaccinated as neonates during that same time period. Nonwhite boys bore a greater risk.
An investigation of infant deaths following initial hepatitis B vaccination based on the Vaccine Adverse Event Reporting System (VAERS), 1992-2002. Soldatenkova, et al. 2007
“In most of the reviewed cases, the history, the symptoms and or the pathologic findings did not support the classification of death as unexplained or SIDS. All cases of “SIDS” occurring shortly after vaccination should be reported to VAERS.
The risks of vaccinating premature, small or slightly ill infants should be weighed against the benefits of each vaccine, particularly in cases where the vaccine is not even needed.
The role of low serum ascorbate in SIDS should be further investigated particularly since the number of recommended pediatric vaccines is constantly increasing.”
Adverse events associated with hepatitis B vaccine in U.S. children less than six years of age, 1993 and 1994. Fisher, et al. 2001
Controlling for age, race, and gender simultaneously in the 1994 NHIS, hepatitis B vaccine was found to be associated with prevalent arthritis [odds ratio (OR) = 5.91, 95% confidence interval (CI) = 1.05-33.14], incident acute ear infections (OR = 1.60, 95% CI = 1.00-2.58), and incident pharyngitis/nasopharyngitis (OR = 1.41, 95% CI = 0.95-2.09).
Recombinant hepatitis B vaccine and the risk of multiple sclerosis: A Prospective Study. Miguel A. Hernán, et al. 2004
Conclusions: These findings are consistent with the hypothesis that immunization with the recombinant hepatitis B vaccine is associated with an increased risk of MS, and challenge the idea that the relation between hepatitis B vaccination and risk of MS is well understood.
Hepatitis B vaccine associated with an increased risk of type 1 diabetes in Italy. P Pozzilli, et al. 2000
The development of rheumatoid arthritis after recombinant hepatitis B vaccination. Pope JE, et al 1998
Recombinant hepatitis B vaccine may trigger the development of RA in MHC class II genetically susceptible individuals.
Cervical intraepithelial neoplasia grade 3 in a patient following Gardasil vaccination. Bruce McLucas, et al. 2019
A 33-year-old woman (Gravida 2, Para 2) received Gardasil in 2006. Subsequently, her pap smear revealed low grade squamous intraepithelial lesion. Cervical biopsies performed in 2015 and 2016 revealed cervical intraepithelial neoplasia grade 1 (CIN 1). She underwent loop electrosurgical excision procedure for persistent CIN 1, which demonstrated CIN 3.
Human papilloma virus-associated squamous cell carcinoma of the larynx in an 18-year-old woman. Hotz MA, et al. 2019
Benign lesion appearance and quadrivalent HPV vaccine status do not exclude HPV-associated malignancies. In our patient, the Gardasil vaccine did not provide crossover protection against HPV 45 infection.
A lowered probability of pregnancy in females in the USA aged 25–29 who received a human papillomavirus vaccine injection. Gayle DeLong. 2018.
Shortly after the vaccine was licensed, several reports of recipients experiencing primary ovarian failure emerged. This study analyzed information gathered in National Health and Nutrition Examination Survey, which represented 8 million 25-to-29-year-old women residing in the United States between 2007 and 2014. Approximately 60% of women who did not receive the HPV vaccine had been pregnant at least once, whereas only 35% of women who were exposed to the vaccine had conceived.
Myasthenia gravis following human papillomavirus vaccination: a case report. Chung JY, et al. 2018
A 23-year-old woman presented with binocular diplopia, ptosis, dysarthria, and dysphagia, which occurred on the 3rd day after the second HPV vaccine administration. She was diagnosed with MG based on history, clinical features, and test results. Her symptoms deteriorated on the 3rd day after admission, and she was transferred to the intensive care unit with mechanical ventilation.
HPV vaccination may cause MG owing to unexpected abnormal autoimmune responses. Additional studies are needed to clarify the possible causal relationship between the HPV vaccine and neurological complications and to evaluate the safety of the vaccine.
Adolescent Premature Ovarian Insufficiency Following Human Papillomavirus Vaccination. Little, et al. 2014
Three young women who developed premature ovarian insufficiency following quadrivalent human papillomavirus (HPV) vaccination presented to a general practitioner in rural New South Wales, Australia. The unrelated girls were aged 16, 16, and 18 years at diagnosis. Each had received HPV vaccinations prior to the onset of ovarian decline.
Human papilloma virus vaccine and primary ovarian failure: another facet of the autoimmune/inflammatory syndrome induced by adjuvants. Colafrancesco S, et al. 2013
We documented here the evidence of the potential of the HPV vaccine to trigger a life-disabling autoimmune condition. The increasing number of similar reports of post HPV vaccine-linked autoimmunity and the uncertainty of long-term clinical benefits of HPV vaccination are a matter of public health that warrants further rigorous inquiry.
Detection of human papillomavirus L1 gene DNA fragments in postmortem blood and spleen after Gardasil® vaccination—A case report. Sin Hang Lee. 2012
A same-nested PCR was used to re-amplify the amplicon of a hypervariable region of the HPV-16 L1 gene DNA in the postmortem blood and splenic tissue obtained at autopsy of a formerly healthy teenage girl who suffered a sudden unexpected death in sleep 6 months after 3 intramuscular injections of a quadrivalent HPV vaccine, Gardasil®. A full autopsy analysis revealed no cause of death.
These naked non-proliferating HPV16 L1 gene DNA fragments appeared to be in the macrophages of the postmortem blood and spleen, and were protected from degradation by binding firmly to the particulate aluminum adjuvant used in vaccine formulation. The significance of these HPV DNA fragments of a vaccine origin found in postmortem materials is not clear and warrants further investigation.
Anaphylaxis following quadrivalent human papillomavirus vaccination. Julia M.L. Brotherton, et al. 2008
From the 269,680 HPV vaccine doses administered in schools, 7 cases of anaphylaxis were identified, which represents an incidence rate of 2.6 per 100 000 doses (95% CI 1.0–5.3 per 100 000). In comparison, the rate of identified anaphylaxis was 0.1 per 100 000 doses (95% CI 0.003–0.7) for conjugated meningococcal C vaccination in a 2003 school-based program.
Based on the number of confirmed cases, the estimated rate of anaphylaxis following quadrivalent HPV vaccine was significantly higher than identified in comparable school-based delivery of other vaccines.
Sudden Infant Death After Vaccination: Survey of Forensic Autopsy Files. Osawa, Motoki MD, PhD et al. 2019
Sudden infant deaths might be attributable to adverse reaction to vaccination, but separating them from coincidental occurrences is difficult…Of the 32 cases in which any vaccines were administered, 7 infants (21.9%) had received immunization within 7 days of death….Judgment of the disorders as truly related to vaccination is difficult, but suspicious cases do exist. Forensic pathologists must devote more attention to vaccination in sudden infant death cases.
Simultaneous sudden infant death syndrome: case report. Y Cevik, et al. 2017. Full text available here:twins dying of SIDS
Both babies had been vaccinated the second doses of oral polio vaccine, diphtheria-pertussis-tetanus and hepatitis B three days before death. The first baby had high fever and was given a full teaspoon (~40 mg) of ibuprofen syrup by the mother. Later, the fever settled according to the mother’s description.
“Infanrix hexa and sudden death: a review of the periodic safety update reports submitted to the European Medicines Agency” Jacob Puliyel, C Sathyamala. 2017
“The number of observed deaths soon after vaccination among children older than one year was significantly higher than that expected by chance once the deleted deaths were restored and included in the analysis.”
Sudden Infant Death With Area Postrema Lesion Likely Due to Wrong Use of Insecticide. Anna M. Lavezzi, et al. 2015
We report a noteworthy case of a 7-month-old infant who suddenly and unexpectedly died during her sleep. After a complete postmortem examination, review of the clinical history, and detailed death scene investigation, the death remained unexplained, leading to a diagnosis of sudden infant death syndrome. However, an extensive review of the brainstem neuropathology revealed a severe alteration in the area postrema (a highly vascular structure lying at the base of the fourth ventricle outside of the blood-brain barrier). The alteration was likely due to massive and repeated to a common household insecticide in the last few weeks of life. These results provide an explanation for this sudden infant death, allowing a differential diagnosis from sudden infant death syndrome.
Gut microbiota and immunity: possible role in sudden infant death syndrome. Paul N. Goldwater. 2015.
The aims of the review are to explore (1) the role of the gut microbiome in relation to the developmentally critical period in which most SIDS cases occur; (2) the mechanisms by which the gut microbiome might induce inflammation resulting in transit of bacteria from the lumen into the bloodstream; and (3) assessment of the clinical, physiological, pathological, and microbiological evidence for bacteremia leading to the final events in SIDS pathogenesis.
“DPT immunization and SIDS”. Kalyani Srinivas, G. Preeti, Sujatha Pasula. 2015
“It is found that mortality with SIDS in the period zero to three days following DTP to be 6.9 times that in the period beginning 30 days after immunization (95 per cent confidence interval, 1.4 to 28)”
“Pesticide exposure during pregnancy, like nicotine, affects the brainstem α7 nicotinic acetylcholine receptor expression, increasing the risk of sudden unexplained perinatal death”. Anna Maria Lavezzi, et al. 2014
We detain that exposition to pesticides in pregnancy produces homologous actions to those of nicotine on neuronal α7-nicotinic acetylcholine receptor, allowing to developmental alterations of brainstem vital centers in victims of sudden unexplained death.
“Sudden twin infant death on the same day: a case report and review of the literature” Huang, et. al. 2013 e.Huang et Twins
[Editors note: Ten week old twin infants received the first doses of oral polio and diphtheria, pertussis, and tetanus (DPT) vaccines 60 days after birth. So day 60 they were vaccinated and they died at 10 weeks, or day 70. Ten days after vaccination, twins died simultaneously on the same night.]
Sudden Infant Death Following Hexavalent Vaccination: A Neuropathologic Study. Matturri, et al. 2013 .Full Text of Hexavalent Vaccination Study
This study does not prove a causal relationship between the hexavalent vaccination and SIDS. However, we hypothesize that vaccine components could have a direct role in sparking off a lethal outcome in vulnerable babies. In conclusion, we sustain the need that deaths occurring in a short space of time after hexavalent vaccination are appropriately investigated and submitted to a post-mortem examination particularly of the autonomic nervous system by an expert pathologist to objectively evaluate the possible causative role of the vaccine in SIDS.
The Initial Common Pathway of Inflammation, Disease, and Sudden Death. Robert M. Davidson and Stephanie Seneff 2012.
Based on extensive review of the scientific literature, we propose in this paper that any exogenous substance that lowers the ZP, and/or introduces polycationic kosmotropic interfacial water stress, and/or lowers the bio-sulfate level, increases the likelihood of sudden death, by triggering a cascade of events in the pathogenesis of inflammation, allergy, infection, thrombosis, hemorrhage, ischemia, infarction, anaphylaxis, disease, and death. Inflammation, allergy, anaphylaxis, and serum sickness should be redefined to reflect this reality. A novel hypothesis as to the etiology of sudden death syndrome is presented which looks specifically at the very earliest events in the pathophysiology of SDS. In most instances, introduction of polycationic surfactants into our bloodstream causes acute interfacial water stress, lowering of ZP, lowering of pH, elevation of viscosity, and electrohemorheologic—hemodynamic derangement. This triggers a cascade of immunologic and hemostatic events, leading inexorably to tissue hypoperfusion, cellular anoxia, seizures, arrhythmias, infarctions, cardiovascular collapse, and death.
“Re-analyses of case-control studies examining the temporal association between sudden infant death syndrome and vaccination”. Ronny Kuhnert, et al. 2012 PDF here Reanalysis of case-control studies examining
“There is no increased or reduced risk of sudden infant death during the period after the vaccination. The previously reported protective effect seen in case control studies is based on the inclusion of unvaccinated cases.”
[Editor’s Note: This study erases any protective effect of vaccines regarding SIDS, because it only came to that conclusion by including a large majority of unvaccinated SIDS cases who died before reaching 2 months old, and thus died before they were eligible for vaccines. A vaccine cannot prevent a death that occurs before a vaccine would be routinely given. However, of infants who lived past 2 months old, they were 4 times more likely to be vaccinated prior to their death. Further research is needed to full understand the mechanism of SIDS, misdiagnosis, and the contributions of vaccines. Explore SIDS here.]
Sudden Unexpected Deaths and Vaccinations during the First Two Years of Life in Italy: A Case Series Study. Giuseppe Traversa, Stefania Spila-Alegiani, et. al. 2011.
Among the 604 infants who died of SUD, 244 (40%) had received at least one vaccination. Four deaths occurred within two days from vaccination with the hexavalent vaccines (RR = 1.5; 95% CI 0.6 to 4.2). The RRs for the risk periods 0–7 and 0–14 were 2.0 (95% CI 1.2 to 3.5) and 1.5 (95% CI 0.9 to 2.4). The increased risk was limited to the first dose (RR = 2.2; 95% CI 1.1 to 4.4), whereas no increase was observed for the second and third doses combined.
Sudden infant death syndrome: a case report in Bosnia and Herzegovina, Dragan Ćajić. 2010
A previously healthy 3 months old, white male infant was found dead after being placed to sleep in the prone position. The features of this case report closely parallel the classical features of SIDS cited in the world literature.
[Editors note: He was vaccinated 5 days before death.]
Cholinergic and oxidative stress mechanisms in sudden infant death syndrome. Anne Dick. 2009
Lower AChE levels and higher combined levels of iron and vitamin C in the first 6 months of life may augment cholinergic and oxidative stress effect, particularly at the age when SIDS is most prevalent. This may contribute to risk of ALTE and SIDS/SUDI events during infancy.
β-Tryptase and quantitative mast-cell increase in a sudden infant death following hexavalent immunization. StefanoD’Errico MargheritaNeri, et al. 2008.
“A fatal case of a 3-month-old female infant, who died within 24 h of vaccination with hexavalent vaccine is presented. Clinical data, post-mortem findings (acute pulmonary oedema, acute pulmonary emphysema), quali-quantitative data collected from immunohistochemical staining (degranulating mast cells) and laboratory analysis with a high level of β-tryptase in serum, 43.3 μg/l, allows us to conclude that acute respiratory failure likely due to post hexavalent immunization-related shock was the cause of death.”
Simultaneous sudden infant death syndrome. Balci Y., et al. 2007
The case(s): Twin girls (3.5-month-old) were found dead by their mother in their crib, both in supine position. The infants were identical twins and delivered at a hospital by cesarean section. Both infants were healthy and did not have any serious medical history. Two days prior to the incident, the twins had received the second dose of oral polio, DPT and the first dose of hepatitis B vaccines and they had fever on the first day of the vaccination and been given teaspoonful of acetaminophen. Death scene investigation, judicial investigation, parental assessment, macroscopic and microscopic autopsy findings and the toxicological analysis did not yield any specific cause of death.
An investigation of infant deaths following initial hepatitis B vaccination based on the Vaccine Adverse Event Reporting System (VAERS), 1992-2002. Soldatenkova, et al. 2007
“In most of the reviewed cases, the history, the symptoms and or the pathologic findings did not support the classification of death as unexplained or SIDS. All cases of “SIDS” occurring shortly after vaccination should be reported to VAERS.
The risks of vaccinating premature, small or slightly ill infants should be weighed against the benefits of each vaccine, particularly in cases where the vaccine is not even needed.
The role of low serum ascorbate in SIDS should be further investigated particularly since the number of recommended pediatric vaccines is constantly increasing.”
Sudden infant death syndrome (SIDS) shortly after hexavalent vaccination: another pathology in suspected SIDS? Giulia Ottaviani, 2006.
Herein we report the case of a 3-month-old female infant dying suddenly and unexpectedly shortly after being given a hexavalent vaccination. Examination of the brainstem on serial sections revealed bilateral hypoplasia of the arcuate nucleus. The cardiac conduction system presented persistent fetal dispersion and resorptive degeneration. This case offers a unique insight into the possible role of hexavalent vaccine in triggering a lethal outcome in a vulnerable baby. Any case of sudden unexpected death occurring perinatally and in infancy, especially soon after a vaccination, should always undergo a full necropsy study according to our guidelines.
Pulmonary immunopathology of sudden infant death syndrome. W.J.HowatBSc, et al. 2003
The results showed three times more eosinophils in the lungs of infants who died of SIDS (27 61 vs 7·91 [99% Cl 1 76-5 87] cells/mm2 for parenchyma) accompanied by increased T lymphocytes and B lymphocytes. These findings provide evidence for an abnormal T lymphocyte-mediated pulmonary inflammatory response in SIDS. Products of eosinophil degranulation can cause epithelial damage and pulmonary oedema, which could cause the respiratory obstruction and hypoxia associated with SIDS.
Simultaneous sudden infant death syndrome: a case report. Ladham S, et al. 2001
The first reported case of simultaneous sudden infant death syndrome (SSIDS) in Allegheny County, Pennsylvania, occurred on February 27, 1998. Two-month-old black fraternal twin girls were both found dead in their crib at the same time. After an in-depth death scene investigation, police investigation, toxicologic analysis, and complete autopsies, a specific cause of death could not be identified. The deaths of the two girls were therefore ruled simultaneous sudden infant death syndrome.
Sudden infant death syndrome and diphtheria‐tetanus‐pertussis‐poliomyelitis vaccination status. Jonville-Bera, et al. 1995
The vaccination status of 118 SIDS and 332 control children, matched for sex, date of birth and age of the victims at death, was compared: the victims of SIDS were not significantly more often vaccinated than control children, the odds ratio was estimated at 1.9 with a 95% confidence interval from 0.9 to 3.9. There was a statistical difference between vaccination status of SIDS cases and controls aged less than three months. Nine percent of SIDS cases under 3 months had been vaccinated whereas the matched controls had not. In our study DTCP vaccination was not a risk factor for SIDS; although more of the SIDS infants less than 3 months of age had been vaccinated.
Involvement of mast cells in sudden infant death syndrome. Platt, MD, et al. 1994
An infant with SIDS had a 20-fold higher chance of having an elevated tryptase level compared with a control infant. Recognition of this pathway as operative in SIDS should facilitate a more precise identification of the allergens involved, the processes leading to mast cell activation, and procedures to identify those infants at risk for anaphylaxis, and should, in time, lead to better therapeutic interventions aimed at preventing this specific cause of SIDS.
Evidence Concerning Pertussis Vaccines and Deaths Classified as Sudden Infant Death Syndrome. Institute of Medicine report 1991
Case reports of SIDS include the deaths of 5- and 10-month-old twins within 3 and 24 hours, respectively, of DPT immunization (Roberts, 1987; Werne and Garrow, 1946). Episodes of death following administration of DPT vaccine were reported for six additional children, five of whom died within 48 hours of immunization (Coulter and Fisher, 1985). Torch (1986) summarized case reports of more than 150 deaths, post-DPT immunization, which had been reported by 37 authors in 12 countries; approximately 50 percent of these deaths occurred within 24 hours, 75 percent within 72 hours, and 90 percent within 1 week following DPT administration. For most of these events, no specific cause of death could be found, and many of these cases were designated as SIDS. (This summary of case reports was published in abstract form only.)
“Diphtheria-Tetanus-Pertussis Immunization and Sudden Infant Death Syndrome”. Walker, et al. 1987
“Focusing on very narrow time intervals following immunization, we found the SIDS mortality rate in the period zero to three days following DTP to be 7.3 times that in the period beginning 30 days after immunization (95 per cent confidence interval, 1.7 to 31).”
Possible temporal association between diphtheria-tetanus toxoid-pertussis vaccination and sudden infant death syndrome. Baraff, et al. 1983
Fifty-three had received a DTP immunization. Of these 53, 27 had received a DTP immunization within 28 days of death. Six SIDS deaths occurred within 24 hours and 17 occurred within 1 week of DTP immunization. These SIDS deaths were significantly more than expected were there no association between DTP immunization and SIDS. An additional 46 infants had a physician/clinic visit without DTP immunization prior to death. Forty of these infants died within 28 days of this visit, seven on the third day and 22 within the first week following the visit. These deaths were also significantly more than expected. These data suggest a temporal association between DTP immunization, physician visits without DTP immunization and SIDS.
a- and B-Tryptase Levels in Near-Miss Sudden Infant Death Syndrome (SIDS) Patients. AD Hogan, MD.
Further evaluation of near-miss SIDS infants with abnormal levels of a and b-tryptase could help to discern which infants are at increased risk of sudden infant death syndrome, and what might cause mast cell activation.
Allergy / Adverse Event Studies
Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disorders. Brian S Hooker, Neil Z Miller. 2020
In this study, which only allowed for the calculation of unadjusted observational associations, higher ORs were observed within the vaccinated versus unvaccinated group for developmental delays, asthma and ear infections. Further study is necessary to understand the full spectrum of health effects associated with childhood vaccination.
Evidence of Increase in Mortality After the Introduction of Diphtheria-Tetanus-Pertussis Vaccine to Children Aged 6-35 Months in Guinea-Bissau: A Time for Reflection? Aaby, Peter, et al. 2018
Although having better nutritional status and being protected against three infections, 6-35 months old DTP-vaccinated children tended to have higher mortality than DTP-unvaccinated children. All studies of the introduction of DTP have found increased overall mortality.
A lowered probability of pregnancy in females in the USA aged 25-29 who received a human papillomavirus vaccine injection. DeLong, Gayle. 2018
Results suggest that females who received the HPV shot were less likely to have ever been pregnant than women in the same age group who did not receive the shot. If 100% of females in this study had received the HPV vaccine, data suggest the number of women having ever conceived would have fallen by 2 million. Further study into the influence of HPV vaccine on fertility is thus warranted.
Childhood vaccine status and correlation with common nonvaccine‐preventable illnesses, Michelle M. Anderson DNP, FNP, 2017.
“Fully immunized group had significantly more ear infections than partial or unimmunized. The unimmunized group had significantly more colds and flu.”
Pilot comparative study on the health of vaccinated and unvaccinated 6- to 12-year-old U.S. children, Anthony Mawson, 2017
“The vaccinated were less likely than the unvaccinated to have been diagnosed with chickenpox and pertussis, but more likely to have been diagnosed with pneumonia, otitis media, allergies and NDD. After adjustment, vaccination, male gender, and preterm birth remained significantly associated with NDD. However, in a final adjusted model with interaction, vaccination but not preterm birth remained associated with NDD, while the interaction of preterm birth and vaccination was associated with a 6.6-fold increased odds of NDD (95% CI: 2.8, 15.5). In conclusion, vaccinated homeschool children were found to have a higher rate of allergies and NDD than unvaccinated homeschool children.”
Three case reports of post immunization and post viral Bullous Pemphigoid: looking for the right trigger. Baroero, et al. 2017
Two of [three cases] developed an eruption of bullous lesions just a few days after vaccination for diphtheria, tetanus, pertussis, poliomyelitis, hepatitis B and Haemophilus influenzae B.
The Allergy Epidemics: 1870–2010. Thomas A.E. Platts-Mills 2016
Since 1990 there has been a remarkable increase in food allergy which has now reached epidemic numbers. Peanut has played a major role in the food epidemic and there is increasing evidence that sensitization to peanut can occur through the skin.
Progressive increase in the recommended immunization of children 1950–2010. The number of injections that children receive in early childhood is a concern for many parents and pediatricians. In addition, several authors have suggested a possible role of these injections in the increase in allergic disease or in food allergy in particular.
History of chickenpox in glioma risk: a report from the glioma international case–control study (GICC). E. Susan Amirian, et al. 2016.
Here, we utilized the GICC data to confirm the previously reported associations between history of chickenpox and glioma risk in one of the largest studies to date on this topic. Using two-stage random-effects restricted maximum likelihood modeling, we found that a positive history of chickenpox was associated with a 21% lower glioma risk, adjusting for age and sex (95% confidence intervals (CI): 0.65–0.96). Furthermore, the protective effect of chickenpox was stronger for high-grade gliomas. Our study provides additional evidence that the observed protective effect of chickenpox against glioma is unlikely to be coincidental.
Who is unlikely to report adverse events after vaccinations to the Vaccine Adverse Event Reporting System (VAERS)? McNeil MM, et al. 2013
The percentage of HCP (Healthcare Providers) aware of VAERS (71%) varied by occupation and primary care practice area. About 37% of HCP had identified at least one AEFI with only 17% of these indicating that they had ever reported to VAERS.
[editors note: 17% OF THE 37% had ever reported to VAERS.]
Increased Risk of Noninfluenza Respiratory Virus Infections Associated With Receipt of Inactivated Influenza Vaccine. Benjamin J. Cowling, et. al. 2012
“We randomized 115 children to trivalent inactivated influenza vaccine (TIV) or placebo. Over the following 9 months, TIV recipients had an increased risk of virologically-confirmed non-influenza infections (relative risk: 4.40; 95% confidence interval: 1.31-14.8). Being protected against influenza, TIV recipients may lack temporary non-specific immunity that protected against other respiratory viruses.”
“Adverse Events following 12 and 18 Month Vaccinations: a Population-Based, Self-Controlled Case Series Analysis.” Kumanan Wilson, et al. 2011
There are significantly elevated risks of primarily emergency room visits approximately one to two weeks following 12 and 18 month vaccination.
Infant mortality rates regressed against number of vaccine doses routinely given: Is there a biochemical or synergistic toxicity? Neil Z Miller and Gary S Goldman. 2011
“Using the Tukey-Kramer test, statistically significant differences in mean IMRs were found between nations giving 12–14 vaccine doses and those giving 21–23, and 24–26 doses. A closer inspection of correlations between vaccine doses, biochemical or synergistic toxicity, and IMRs is essential.”
Frequency of allergic diseases following measles. E. Kucukosmanoglu, et al. 2006.
The results of this study indicate that findings of allergic disease are less frequent in children with a history of measles.
“The relationship between vaccine refusal and self-report of atopic disease in children”. Rachel Enriquez, PhD. 2005
“Parents who refuse vaccinations reported less asthma and allergies in their unvaccinated children.”
Asthma and vaccination history in a young adult cohort. G. Benke, M. Abramson. 2004
However, subjects reporting full immunisation were found to be at higher risk to asthma (RR 1.52, 95% CI 1.09-2.11) but not atopy. Conclusions: Our results show relatively weak support for the hypothesis that childhood vaccinations may lead to increased risk of asthma, but caution is advised due to possible recall bias.
“Vaccination and Allergic Disease: A Birth Cohort Study” Tricia M. McKeever, PhD, 2004.
“Our univariate analysis showed that exposure to DPPT was associated with an increased risk of developing asthma (hazard ratio [HR] = 14.0; 95% confidence interval [CI] = 7.3, 26.9) and eczema (HR = 9.40; 95% CI = 5.92, 14.92)”
In this observational study analyzing computerized primary care records, we found an association between MMR and DPPT vaccination and the incidence of asthma and eczema, but these associations appeared to be limited to the minority of children who rarely seek care from a GP. This limited association is more likely to be the result of bias than a biological effect.”
[Editor’s Note: when an association is found between vaccination and allergy, it is considered bias, because they are so healthy, because they are unvaccinated, that they do not need to see a doctor.]
Symptoms after accelerated immunisation. Mary E B Ramsay, 1992.
[Editor’s note: Out of 107 infants, had reactions to vaccines that compelled the parents to not continue with the pertussis component of the vaccine:
“Only one of the children had a genuine contraindication to further doses of pertussis vaccine, when he developed a temperature of 40.5°C (104.9 degrees F) on evening 2 after vaccination (measured by the mother). The second child was afebrile but seemed distressed with a high pitched cry on the first evening. Although the crying was neither prolonged nor inconsolable and therefore did not constitute a contraindication to further pertussis vaccine, the mother opted to complete with diphtheria-tetanus only vaccine.”
[Editor’s note: We are told that vaccine reactions are “one in a million” and in this study of 107 infants, 2 reportedly had reactions that warranted caution, and exempted at least one of the infants from further vaccination.]
Confounding in Studies of Adverse Reactions to Vaccines, Paul Fine, 1992.
Most published studies have reported a deficit of sudden infant death syndrome among vaccinees, which may reflect confounding in their study designs. An expression is derived to explore the extent of underestimation that may be introduced in such studies, under different sets of conditions. Confounding of this sort is a general problem for studies of adverse reactions to prophylactic interventions, as they may be withheld from some individuals precisely because they are already at high risk of the adverse event.
Evidence Concerning Pertussis Vaccines and Central Nervous System Disorders, Including Infantile Spasms, Hypsarrhythmia, Aseptic Meningitis, and Encephalopathy, Institute of Medicine (US) Committee to Review the Adverse Consequences of Pertussis and Rubella Vaccines; Howson CP. 1991
The evidence is consistent with a causal relation between DPT vaccine and acute encephalopathy,3 defined in the controlled studies reviewed as encephalopathy, encephalitis, or encephalomyelitis.
Anemia of a mild viral infection: the measles vaccine as a model. Olivares M. 1989.
93 infants were immunized with live attenuated measles virus and studied prospectively at 0, 4, 9, 14, 21, and 30 days. Hemoglobin concentration decreased significantly by days 9 and 14. The decrease was greater than 1.0 g/dL in 8.6% and greater than 0.6 in 24.3% of the infants. Of the nonanemic infants, 22% became anemic.
Aluminum / Adjuvant Studies
Oral exposure to aluminum leads to reduced nicotinic acetylcholine receptor gene expression, severe neurodegeneration and impaired hippocampus dependent learning in mice. Mehpara Farhat S, et al. 2019
Aluminum (Al) is known for its neurotoxicity for over a century and is reported to have specifically high toxicity for cholinergic system… These results demonstrated that Al exposure caused neurotoxicity in mice hippocampus which is manifested by reduced memory and elevated anxiety. The results were further validated by high Al accumulation in the hippocampus, severe neurodegeneration and reduced expression of nAChRs.
“Aluminium in brain tissue in autism”. Mold M, Umar D, King A, Exley C. 2018
“The pre-eminence of intracellular aluminium associated with non-neuronal cells was a standout observation in autism brain tissue and may offer clues as to both the origin of the brain aluminium as well as a putative role in autism spectrum disorder.”
Aluminium in Brain Tissue in Multiple Sclerosis. Matthew Mold, et al. 2018
The aluminium content of brain tissue in MS was universally high with many tissues bearing concentrations in excess of 10 μg/g dry wt. (10 ppm) and some exceeding 50 ppm. The association of aluminium with corpora amylacea suggests a role for aluminium in neurodegeneration in MS.
Synergism in aluminum and mercury neurotoxicity. Peter N Alexandrov, Aileen I Pogue. 2018
“This is the first report on the neurotoxic effects of aluminum sulfate and/or mercury sulfate on the initiation of inflammatory signaling in human brain cells in primary culture. The effects aluminum+mercury together on other neurologically important signaling molecules or the effects of other combinations of common environmental metallic neurotoxins to human neurobiology currently remain not well understood but certainly warrant additional investigation and further study in laboratory animals, in human primary tissue cultures of CNS cells, and in other neurobiologically realistic experimental test systems.”
“Non-linear dose-response of aluminium hydroxide adjuvant particles: Selective low dose neurotoxicity”. Crépeaux G, et. al. 2017
An unusual neuro-toxicological pattern limited to a low dose of Alhydrogel® was observed. Neurobehavioural changes, including decreased activity levels and altered anxiety-like behaviour, were observed compared to controls in animals exposed to 200μg Al/kg but not at 400 and 800μg Al/kg…..We conclude that Alhydrogel® injected at low dose in mouse muscle may selectively induce long-term Al cerebral accumulation and neurotoxic effects.
“The putative role of environmental aluminium in the development of chronic neuropathology in adults and children. How strong is the evidence and what could be the mechanisms involved?”. Gerwyn Morris, Basant K. Puri, and Richard E. Frye. 2017
“Exposure to Mercury and Aluminum in Early Life: Developmental Vulnerability as a Modifying Factor in Neurologic and Immunologic Effects.” José G. Dórea. 2015
“Currently, ethylmercury (EtHg) and adjuvant-Al are the dominating interventional exposures encountered by fetuses, newborns, and infants due to immunization with Thimerosal-containing vaccines (TCVs). Despite their long use as active agents of medicines and fungicides, the safety levels of these substances have never been determined, either for animals or for adult humans—much less for fetuses, newborns, infants, and children……More research attention has been given to EtHg and findings have showed a solid link with neurotoxic effects in humans; however, the potential synergic effect of both toxic agents has not been properly studied. Therefore, early life exposure to both EtHg and Al deserves due consideration.”
“Effect of Routine Vaccination on Aluminum and Essential Element Levels in Preterm Infants.” Tammy Z. Movsas 2013
No significant change in levels of urinary or serum aluminum were seen after vaccination. Significant declines were noted postvaccination in serum iron (58.1%), manganese (25.9%), selenium (9.5%), and zinc (36.4%) levels, as was a significant increase in serum copper level (8.0%). A rise in selenium level was the only significant urine change.
[Editor’s note: An increase in post-vaccination serum or urine levels of Aluminum was not detected because Aluminum adjuvants are not excreted, which lends further support to the hypothesis that Aluminum adjuvants bioaccumulate and translocate to other parts of the body, for example, the brain.]
“Mechanisms of aluminum adjuvant toxicity and autoimmunity in pediatric populations”. Tomljenovic L, Shaw CA. 2012
“Autoimmunity following hepatitis B vaccine as part of the spectrum of ‘Autoimmune (Auto-inflammatory) Syndrome induced by Adjuvants’ (ASIA): analysis of 93 cases”. Zafrir Y, Agmon-Levin N, Paz Z, Shilton T, Shoenfeld Y. 2012
Aluminum Adjuvant Linked to Gulf War Illness Induces Motor Neuron Death in Mice, Michael S. Petrik. 2007.
The findings suggest a possible role for the aluminum adjuvant in some neurological features associated with GWI and possibly an additional role for the combination of adjuvants.
Systemic inflammatory reaction after pneumococcal vaccine. Kelley A von Elten, et al. 2014
Fever, leukocytosis, and large local reactions following the pneumococcal polysaccharide vaccine (PS23) have been described only in isolated case reports in the adult literature.
Protracted fever with cellulitis-like reaction in pneumococcal polysaccharide-vaccinated children. Daniel Tsung-Ning Huang 2008.
Side effects of the 23-valent pneumococcal polysaccharide vaccine (PPV23) are regarded as mild and uncommon in adults. In our clinical experience, however, protracted fever with a cellulitis-like reaction after PPV23 vaccination is not rare in pediatric patients. We reviewed the records of 17 children with those clinical findings after PPV23 vaccination.
Rotavirus shedding following administration of RV3-BB human neonatal rotavirus vaccine. Cowley, et al. 2017
Shedding of rotavirus was highest following vaccination at 8 weeks of age in both neonatal and infant schedules (19/30 and 17/27, respectively). Rotavirus was detected in stool on days 3–7, after at least one dose of RV3-BB, in 70% (21/30) of neonate, 78% (21/27) of infant and 3% (1/32) placebo participants.
Risk of Intussusception After Rotavirus Vaccination A Systematic Literature Review and Meta-Analysis. Judith Koch, Dr. 2017
RV vaccination is associated with a markedly elevated RR and a mildly elevated AR for intussusception 1–7 days after the first dose. Physicians should begin the series of vaccinations at age 6–12 weeks, as recommended by the STIKO, because the risk of intussusception is higher afterward. Current health insurance company claim data indicate that 11.2% of infants are still receiving the first dose of the vaccine at ages above 3 months. The parents of vaccinated children should be informed about the possible signs of intussusception (colicky pain, bilious vomiting, and red “currant jelly” stool).
Comparison of virus shedding after lived attenuated and pentavalent reassortant rotavirus vaccine. Yu-Chia Hsieh, et al. 2014
After the first vaccine dose, the peak time of virus shedding occurred between day 4 and day 7, with positive detection rates of 80-90% by real-time RT-PCR and 20-30% by EIA. In both groups, vaccine shedding occurred as early as one day and as late as 25-28 days.
An analysis of rotavirus vaccine reports to the vaccine adverse event reporting system: more than intussusception alone? Penina Haber, et al. 2004
Even after excluding intussusception cases, a higher proportion of RRV-TV reports than non-RRV-TV reports included fever and various gastrointestinal symptoms, most notably bloody stool but also vomiting, diarrhea, abdominal pain, gastroenteritis, abnormal stool, and dehydration.
Intussusception and gastroenteritis were the most commonly reported outcomes; however, a substantial number of reports indicate signs and symptoms consistent with either illness, possibly suggestive of a spectrum of gastrointestinal illness(es) related to RRV-TV.
Zoster vaccine-associated primary varicella infection in an immunocompetent host. Kaoru Harada, et al. 2017
A 64-year-old immunocompetent man developed a widespread pruritic and vesicular rash 2 weeks after receiving the zoster vaccine (Zostavax). He had fever, bandaemia with normal total white blood cell count and mild transaminitis. PCR testing of serum and skin was positive for varicella zoster virus (VZV), while serum VZV IgG was negative.
Varicella Zoster Virus DNA at Inoculation Sites and in Saliva After Zostavax Immunization. Duane L Pierson 2011
Analysis of 36 individuals over age 60 years who were immunized with Zostavax revealed varicella zoster virus (VZV) DNA in swabs of skin inoculation sites obtained immediately after immunization in 18 (50%) of 36 subjects (copy number per nanogram of total DNA, 28 to 2.1 × 106) and in saliva collected over 28 days in 21 (58%) of 36 subjects (copy number, 20 to 248). Genotypic analysis of DNA extracted from 9 random saliva samples identified vaccine virus in all instances. In some immunized individuals over age 60, vaccine virus DNA is shed in saliva up to 4 weeks.

Young Girl Wheelchair Bound After Merck’s Gardasil, Mom Sues
Sydney Figueroa was a happy, healthy, vibrant 11 year old Pennsylvania girl when she received the

Mother of 10 Year Old Girl Who Developed Fatal Disease After Gardasil Sues Merck
The parents of a North Carolina girl have filed a wrongful death lawsuit after their daughter,

Toddler Dies 30 Hours After 3 Shots: MMR, Varicella and Hep A Vaccinations
Shared from his mother, Gabriella. “Hi my name is Gabriella, the mother of Dino Angelo Santuccione,

TikTok Influencer’s Baby Cash Died In His Sleep A Few Days After ‘6 Week Shots’
Australian TikTok influencer Veruca Salt, whose real name is Kimberley Summer Hartley, 25, has shared the

15 Month Old Toddler Dies 2 Days After ‘Well-Visit’ Vaccinations
In the State of New York, infants and children are required to be vaccinated against ten

Baby Died of SIDS Three Days After Vaccinations
Kari Bundy is a warrior mom. Like so many mothers before and after her, Kari trusted

Baby Dies 34 Hours After Vaccines
In October 2022, Melissa, a registered nurse, brought her infant son to the pediatrician for a

Vaccines and the Premature Infant
We all want to make it to 39 or 40 weeks, but sometimes life has different

SUDC After Vaccines
Every year in the United States around 400 children between the ages of one and 18

Did the Mysterious Medical Condition in Take Care of Maya Begin After an HPV Vaccine?
The new Netflix documentary Take Care of Maya tracks the heartbreaking and enraging medical kidnapping story of

The Vaccine Schedule Through The Years
It’s hard to believe, but the very first CDC pediatric vaccine schedule was only introduced in

Vaccine Deaths In Children and Infants
Last night I watched a home improvement show and was bombarded with pharmaceutical ad after pharmaceutical
