











How Maine’s Infant Mortality Rate Reflects Larger Issues Nationwide
Recently Maine has been making headlines for some very different reasons. First off, the state was heralded for having the highest rate of toddler vaccinations out of the country, taking first place for having the largest percentage of children between 19 and 35 months old vaccinated with at least one dose of MMR (measles, mumps and rubella), DTaP (diptheria, tetanus and whooping cough) and varicella (chickenpox) shots, according to the most recent map released by The American Academy of Pediatrics.
Yet tragically, at the same time, the state is also scrambling to figure out why its infant mortality rate is increasing. Out of 50 states, it is the only state whose infant mortality rate (IMR) is on the rise. And to add more confusion, just a few short years ago, it had the lowest IMR out of all 50 states. In 2016, Maine ranked no. 39.

Click here for the IMR interactive map.
Dr. Dora Anne Mills wrote in her article for the Portland Press Herald, “infant mortality – the rate at which babies die in the first year of life – is the most accurate pulse we have on the health of a society.” I couldn’t agree with her more.
In 2016, Maine’s rate of infant mortality was 6.9 deaths per 1,000 live births, much higher than any of its New England neighbors, and higher than the national average of 5.1 deaths per 1,000 live births. Keep in mind the United State’s IMR is–without any sugar coating–completely awful. Germany, Japan, Sweden, Lithuania, Iceland, Austria, Spain, Italy, Israel, Ireland, Taiwan, Cuba, Australia, Hungary, Canada–all have lower IMR’s than good old United States.
 According to the CIA World Fact Book, the United States ranks no. 56 for Infant Mortality, meaning 55 countries have fewer infant deaths in the first year of life for every 1,000 live births, each year. Our nation is sandwiched right in between Serbia, and Bosnia and Herzegovina. The United States spends more money on healthcare than any other country–how could the United States have a lower life expectancy, higher maternal mortality, and higher infant mortality rate than dozens of so many highly developed nations.
According to the CIA World Fact Book, the United States ranks no. 56 for Infant Mortality, meaning 55 countries have fewer infant deaths in the first year of life for every 1,000 live births, each year. Our nation is sandwiched right in between Serbia, and Bosnia and Herzegovina. The United States spends more money on healthcare than any other country–how could the United States have a lower life expectancy, higher maternal mortality, and higher infant mortality rate than dozens of so many highly developed nations.
The United States also has more preterm birth than 53 countries. Preterm birth is a leading cause of death and a major risk factor for both SIDS and Autism. No matter how you slice it–our nation’s infant mortality rate is an embarrassment, and more importantly, an indication that something is very, very wrong. Sadly, Maine isn’t the only one with a problem.
Like two sides of a spinning coin, the simultaneity of such conflicting headlines: “high vaccination rates” and “increasing infant mortality” is perplexing. How can two seemingly divergent realities co-exist in the same space? Research scientists Neil Z. Miller and Gary S. Goldman wondered the same thing in 2011 when they explored how countries with high mortality rates have more vaccine doses given to their infants in the first year of life.
“The US childhood immunization schedule specifies 26 vaccine doses for infants aged less than 1 year—the most in the world—yet 33 nations have lower IMRs.”
Even today, no country surpasses our immunization schedule in number of doses or number of required vaccines.
And despite the spending on health care, and large number of vaccine doses, our infants and children are not healthier.
In their study, Miller and Goldman wondered if there was a biochemical or synergistic toxicity to today’s vaccine schedule that conducted the higher IMR. I’m wondering if there is a synergistic toxicity with all forms and routes of chemical exposure–from routine immunizations to pesticides and every single chemical we come in contact with every day that has unexpected consequences in developing fetuses and infants?
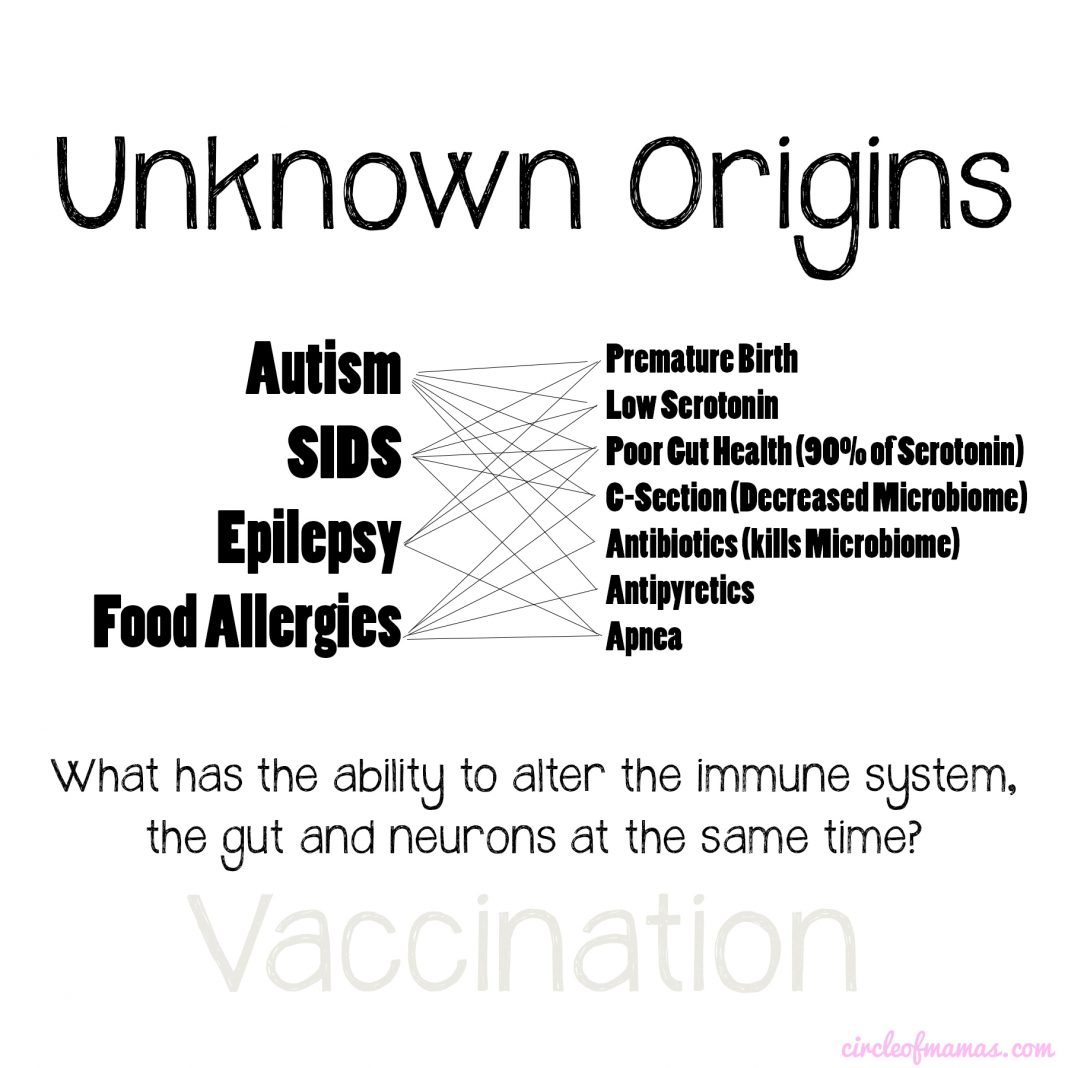
Could total external and internal toxin exposure have cumulative mutagenic effects on DNA? What is the mechanism that creates the autoantibodies we observe in a number of immune related diseases and syndromes? Are we playing a role in creating both the genetic and environmental conditions resulting in the rise of unexplained birth defects, SIDS, food allergies, epilepsy and other seizure disorders, autism, ADHD, Apraxia, and other forms of neurological and immune system damage?
Are the clinical trials and observational studies in charge of assessing vaccine safety missing key data by conducting studies on babies who are 1. Healthy and not premature; 2. Who are not living in GMO agricultural regions; 3. Who are not exposed to similar chemical and environmental contaminants and pollution; 4. Who are not residing in countries with mandatory folic acid fortification in place; and 5. Whose pregnant women are not recommended the same medications and vaccines while pregnant at the same frequencies.

Leading Causes of Infant Death
The leading causes of infant death are not from vaccine preventable diseases, although the governmental push to vaccinate every living, breathing thing would have you think otherwise. More than 23,000 babies died in the United States in 2014. The leading causes of infant death were and are: birth defects; premature birth/low birthweight; SIDS; respiratory distress syndrome; and maternal complications of pregnancy.
According to March of Dimes:
-
In Maine in 2013, 91 infants died before reaching their first birthday, an infant mortality rate of 7.1 per 1,000 live births.
-
Between 2003 and 2013, the infant mortality rate in Maine increased more than 39%.
-
In 2013, 60.4% of infant deaths occurred in the neonatal period, and 39.6% occurred in the postneonatal period.
Are the Kids All Right?
Just a little over a decade ago, Maine had the lowest IMR out of the nation: ranking no. 1 for least infant deaths per 1,000 live births for both 1996 and 2002. After that something changed. By 2013, Maine dropped to 44th place, and then barely recovered up to 37th in 2014. That year, the CDC announced Maine had the highest vaccination rates for 19-35 month old children in the nation. But how did the state go from the lowest mortality rate to highest in a matter of a few years? Today, Maine’s infant mortality rate of 6.9 infant deaths (age under one) per 1,000 live births, and is on par with third world countries.
While Maine’s more southern and urban infant mortality rates have for the most part stayed the same, most of Maine’s rural counties have worsened. It’s worth noting that the more urban counties have higher rates of exemptions from vaccines and correspondingly lower IMR. Piscataquis County has an unusually high rate, hovering around 13.2 deaths per 1,000 live births in 2015 and 15.8 deaths per 1,000 live births in 2014. That county is the least populated county, with an overall population of 17,000. That county had a very low infant mortality rate of 2 or 3 deaths per 1,000 live births up until 2009.
From 2009 to 2015, Piscataquis County’s IMR rose 164%. By contrast, Nearby Aroostook County and Penobscot County rose 12% and 21% over the same years, respectively. But to make it more confusing, Piscataquis county only had 134 births in 2014, for example. So that means they had 1 or 2 deaths. They have one hospital and three schools.

Similar to national trends in IMR, the leading causes of infant deaths in Maine between 2008 and 2010 were: 1. Disorders related to short gestation and low birth weight; 2. Congenital malformations, deformations and chromosomal abnormalities; 3. Newborn affected by complications of placenta, cord and membranes; 4. Unintentional injuries; 5. Sudden Infant Death Syndrome (SIDS).
In 2009, during the H1N1 pandemic flu season, Maine’s public health nurses managed to vaccinate children and seniors at the highest rates in the nation. Many pregnant women around the country were encouraged to get this flu shot, resulting in an increase of fetal loss reports to VAERS, that spawned many studies, many attempting to exonerate the H1N1 vaccine in pregnant women, but some found an increase in birth defects and preterm birth for exposed infants in the first trimester of pregnancy, which is a trimester that most of the other studies leave out of their findings.
Is Poverty in Rural Maine to Blame?
Dr. Mills’ article focused entirely on poverty as a possible explanation for the rising IMR. According to March of Dimes, the majority of infant deaths fall into these five categories:
Leading Causes of Infant Deaths
-
Birth Defects
-
Prematurity/Low Birthweight
-
Sudden Infant Death Syndrome
-
Respiratory Distress Syndrome
-
Maternal Complications of Pregnancy
These causes can happen to anyone, anywhere, in every financial situation. Lack of health care is not an explanation, because every expectant mother in Maine (and the rest of the country) with low income is automatically eligible for each state’s Medicaid program. In Maine it’s called MaineCare, and it provides free or low-cost health insurance for families with children and pregnant women. Women may start prenatal care immediately with MaineCare.
Poverty may be a risk factor (because of unsanitary living conditions and poor diet), but poverty in and of itself doesn’t explain a rising infant mortality. While it’s true, some of the rural counties in Maine have up to 25% of children living within the federal guidelines of poverty (which is defined as a family of four earning less than $28,000 per year), take California for example, a very large number of counties have more than 25% of children living within the federal guidelines of poverty, yet California’s IMR is still much lower at an average of 4.5 per 1,000 live births. Poverty wise, they are not too different.
It was estimated for 2015, that 13.4% people were living in poverty in Maine, accounting for 172K people living below the poverty limit, which is considered a family of four earning less than $24K per year. By contrast, California’s poverty estimate for 2015 was 15.3%, accounting for 5.8 million people living below the poverty limit. California’s poverty level is technically higher, and yet the state’s IMR is well below Maine’s.

Mississippi, First in IMR and Vaccinations
Mississippi, which is one of three states that has removed all vaccine exemptions except medical, has the highest infant mortality rate and highest rate of premature infant deaths out of any state. Prematurity is a major cause of infant deaths. Incidentally, the state also has the highest rate of vaccination for school-aged children. In Mississippi, the IMR for African American babies is twice the rate as non-hispanic white babies. The discrepancy could be due to genetic susceptibility–Autism, SIDS, Premature birth are all more prevalent in African American and American Indian infants and children, especially boys. The rate of non-hispanic white infants in Mississippi is 6.8 deaths per 1,000 live births, which is actually the same rate in Maine. New Hampshire and Vermont by comparison both have lower IMR: 4.4, while Massachusetts has 3.5 deaths per 1,000 live births for non-hispanic white infants. As far as infant mortality is concerned, Maine sticks out like a sore thumb. 
Hundreds of miles from the deep south, why would Maine have more in common with Mississippi than its own New England neighbors? Mississippi has the highest vaccination rate for school-aged children in the country. California just recently joined Mississippi and West Virginia with removing personal belief exemptions to vaccination in 2016.
Maine’s neighbor, New Hampshire, has half the rate of birth defects, and less premature infants and slightly fewer deaths from maternal complications. It shares a border with Maine. New Hampshire also has half the rate of autism.

West Virginia is the other state that only has medical exemptions.

Let’s Talk About Birth Defects
According to the CDC, one in every 33 babies born in the United States is born with a birth defect (about 3% of all babies). Birth defects are the leading cause of infant deaths, accounting for 20% of all infant deaths.
According to March of Dimes:
“Every year an estimated 8 million children–6 percent of total births worldwide–are born with a serious birth defect of genetic or partially genetic origin. Additionally, hundreds of thousands more are born with serious birth defects of post-conception origin due to maternal exposure to environmental agents. At least 3.3 million children less than 5 years of age die annually because of serious birth defects and the majority of those who survive may be mentally and physically disabled for life.”
Right there in plain sight: Birth defects are a result of maternal exposure to environmental agents. Each year, 120,000 babies are affected by birth defects in the United States. Toxin exposure can produce identifiable birth defects, but can also stimulate changes in the brain that we can’t see. Infants who died of SIDS were found to have abnormal brain stems and low serotonin and fewer serotonin receptors, which we know from studies comparing autopsied brains of babies who died of SIDS and comparing them to babies who died of known causes. What was able to make changes to their brain at the neuronal level?
A Clean and Healthy Pregnancy
There is a laundry list of chemicals to stay away from when pregnant to prevent birth defects. This is why we don’t smoke or drink alcohol, and why we use low voc paint in our baby’s nursery, and why we aren’t supposed to eat too much tuna. We are told to stay away from hazardous substances like lead, mercury, PCBs, carbon monoxide, paint, dioxin and pesticides. And we think we are. But there are a lot of unknowns. What about the substances and medications that are generally recognized as safe? What about the drugs given to us by our doctors? What about Tylenol, the flu shot, Tdap, Folic Acid supplementation, and antidepressant medication during pregnancy?
We all probably assume substances like “lead” are a thing of the past right? Oh my gosh, sadly, we are wrong. Any home or building built before 1986 is likely to have lead pipes, fixtures and solder. Lead can enter drinking water when service pipes that contain lead corrode, especially where the water has high acidity or low mineral content that corrodes pipes and fixtures. You know what the EPA says is the safe level of lead to have in drinking water? ZERO. Because lead is a toxic metal that can be harmful to human health even at low exposure levels. Lead is persistent, and it can bioaccumulate in the body over time. Lead is neurotoxic at every exposure level.
Your city’s water quality report is one thing, but your house and your child’s daycare facility or school is another. Just in the last year, schools and daycare facilities all. over. the. country, including Maine, are turning off drinking fountains because of dangerously high levels of lead. What kind of water is in your baby’s bottle or sippy cup?
A recent study looking at the baby teeth of twins with and without Autism found dangerously high levels of lead in the Autistic children’s teeth during specific intervals, especially during the months just before and right after they were born, up until about 15 weeks old. What happens to most babies right before they are born, and right after they are born? Hello Tdap, epidural, Hep B, Vitamin K, and two- and four-month vaccinations. Lead was detected in measurable amounts in the commonly used vaccine adjuvant aluminum hydroxide, which is a key ingredient in Tdap, Hep B, and most of the CDC recommended pediatric vaccine schedule. Lead and other heavy metal contamination was also discovered in every pediatric vaccine these Italian scientists tested. Despite our best efforts, we fail. Because we don’t target the problem at its head.
Birth defects are not decreasing, in fact most are increasing. Gastroschisis, a serious birth defect where a baby’s intestines stick outside of the body through a hole beside the belly button, is on the rise according to the CDC, and most prevalent among young mothers under the age of 20. A very common birth defect, cleft lip, is associated with having genetic mutations in the MTHFR pathway. It is estimated that nearly 20% of the population carries at least one of the MTHFR mutations. Infants carrying this mutation can have fatal outcomes with use of general anesthesia. How many premature infants and infants undergo surgery every year with or without birth defects, with or without this mutation and don’t survive? We do not routinely perform genetic testing on infants prior to surgery. Maybe we should.
Why is SIDS Still Unexplained?
Our attempts to lower infant mortality or prevent birth defects have leveled off because once again, we are treating the symptoms not changing the conditions. Our tactics do not address the larger picture but only the risk factors. The “Back to Sleep” campaign reduced SIDS, while we saw an increase in deaths attributed to “suffocation” and “unknown cause”. Thereby making SUIDs level off around 1996. Folic acid fortification initially reduced neural tube defects, which then leveled off quickly, similar to “Back to Sleep”. Too much synthetic folic acid has been associated with autism, and is dangerous to people with MTHFR mutations. Despite our best efforts, we lack fundamental understanding.


It’s every parent’s worst nightmare. Your perfectly healthy baby just doesn’t wake up one day. It could happen to anyone. And some times the baby isn’t even asleep. Parents are not given an explanation, because there is no single agreed upon etiology of SIDS.
SIDS (Sudden Infant Death Syndrome) is a subset of SUID (Sudden Unexplained Infant Death). In 2015, there were about 3,700 sudden unexpected infant deaths in the United States, which fall into three categories: SIDS, Unknown Cause, and Accidental Suffocation and Strangulation in Bed. SIDS is the leading cause of death among infants 1 to 12 months old. About 1,600 infants died of SIDS in 2015.
 Preterm birth, being small for gestation age, stomach sleeping, cigarette smoking in the home, a respiratory infection–these are risk factors for SIDS. Being male, African American, and American Indian are also risk factors. Most instances of SIDS occur when an infant is between two and four months old, around the time of the two- and four-month vaccines.
Preterm birth, being small for gestation age, stomach sleeping, cigarette smoking in the home, a respiratory infection–these are risk factors for SIDS. Being male, African American, and American Indian are also risk factors. Most instances of SIDS occur when an infant is between two and four months old, around the time of the two- and four-month vaccines.
Research scientists are putting the pieces together for SIDS. Infants who are sleeping prone have a harder time to rouse in an episode of apnea, and are more likely to not recover from an upper airway obstruction. But back sleeping doesn’t address the cause of apnea, the cause of low serotonin (90% of serotonin is manufactured in the gut), and the changes to the serotonin receptors.
The European flu vaccine Pandemrix caused narcolepsy is some individuals by eliciting antibodies to the part of their brain that controls sleep. Similarly, the presence of autoantibodies have been detected in mothers and children with autism, that target specific areas and receptors in the brain of the developing fetus. The presence of autoantibodies have been documented in full term, otherwise healthy, stillbirths. Autoantibodies can be induced by vaccination in susceptible individuals. The H1N1 vaccine was observed to have stimulated more anticardiolipin antibodies verses the seasonal influenza vaccine, which is the same antibody found in this stillborn’s mother. It is known Infants who died of SIDS were found to have less serotonin and serotonin receptors in their brains–could autoantibodies be contributing to this brain abnormality? If SIDS is determined to be autoimmune in nature, the question should be, should we be interfering with the immune system?
Preterm birth is implicated as a risk factor for a number of syndromes, including Autism and SIDS. According to the CDC, Maine ranked 46th for pre-term birth in 2013, with a rate of 9.3%, and had around 7% of infants being born with low birth weight. Thirty percent of total births are delivered via cesarean section. Premature and low birth weight babies are recommended to be vaccinated on the same schedule as full-term babies, despite there being studies that show it increases cardiorespiratory events, apnea, bradycardia, and sepsis workups.

 From 2001-2003, Maine had an average rate of 38.9 SIDS deaths per 100k live births that jumped in ten years to 62.7 deaths per 100k live births, higher than the national average of 43.4 deaths per 100k live births. By contrast, California’s rate of SIDS only rose from 27.2 deaths to 32.4 deaths per 100k live births in the same 10 year period. SIDS accounted for 9% of all infant deaths in Maine in 2011-2013.
From 2001-2003, Maine had an average rate of 38.9 SIDS deaths per 100k live births that jumped in ten years to 62.7 deaths per 100k live births, higher than the national average of 43.4 deaths per 100k live births. By contrast, California’s rate of SIDS only rose from 27.2 deaths to 32.4 deaths per 100k live births in the same 10 year period. SIDS accounted for 9% of all infant deaths in Maine in 2011-2013.
Autism, ADHD Also Increasing in Maine
Autism is on the rise everywhere in the United States, but especially so in Maine. In 2000, Maine’s school system was serving just under 600 students with autism. By 2009, that number climbed to 2,471 students with autism. Then in 2013, that number climbed to 3,097. This represents a 416% increase in 13 years. Perhaps there are more people taking advantage of special education services or perhaps guidelines for qualifying for an autism diagnosis has expanded, but Maine had the highest rate of autism for 3-5 year olds out of any state. And if it’s not first, it’s definitely in second place for most children diagnosed as autistic.
In the 2015-2016 school year, 17% of Maine’s public school students were receiving special education services. California by contrast served about 11.5% of the K-12 population with special education services.
One thing to keep in mind when talking about the etiology of autism, is the area of epigenetics. Scientists recently discovered that if a girl’s maternal grandmother smoked during pregnancy, the girl is 67% more likely to display certain traits linked to autism, such as poor social communication skills and repetitive behaviors. Some of the health effects we are seeing today could have been sewn generations ago, when lead was in household paint, when pregnant women smoked without stigma, when asbestos was the floor tile your mother or grandmother played on.

In addition to high rates of autism, Maine experienced a surge in ADHD treatment, reporting a 35% growth rate from 2008 to 2010, ranking the state #5 in the nation. Maine’s rate growth for ADHD during those years was twice the national average of 17 percent.
In Maine, 13% of children had ADD or ADHD in 2011. Among all children age 4 to 17 in Maine, 6.6 percent are taking medication for the disorder, according to the CDC.
Youth Aged 4-17 Ever Diagnosed with Attention-Deficit
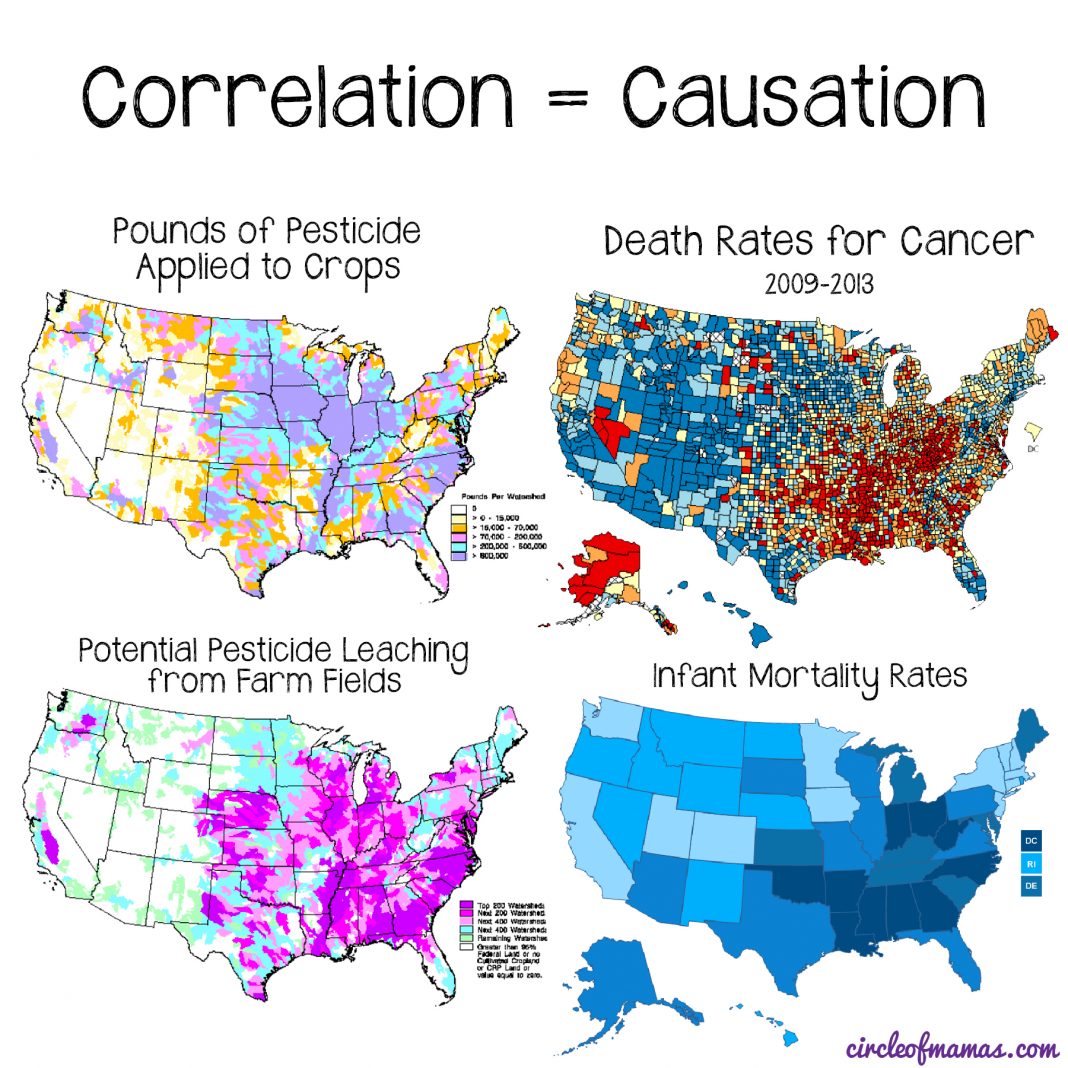
 Astonishingly, the CDC’s own ADHD prevalence map lines up with the Cancer Mortality map, the USDA’s pesticide map, and the Infant Mortality map.
Astonishingly, the CDC’s own ADHD prevalence map lines up with the Cancer Mortality map, the USDA’s pesticide map, and the Infant Mortality map.
Learn From the Past, Change the Future
Honey, we are doing it again. We did it with Thalidomide. We did it with Primodos. We do it when we perform unnecessary c-sections and when we give a premature infant too many vaccines. We thought glyphosate was safe because the “science was settled”, but now information has surfaced that the EPA may have been in cohoots with Monsanto, the major manufacturer of glyphosate, actively discounting the pesticide’s cancer risks.
There is no question that pesticides and chemicals play a role in these interconnected, widespread epidemics. There is no question that vaccines play a role. The question is how? And what can we do to change our future, our children’s future, our grandchildren’s future?










